INTRODUCTION
The advancement of artificial intelligence (AI) and virtual reality (VR)/augmented reality (AR) technologies has progressed from the initial stages of simple digital healthcare to actively preventing and treating diseases through digital therapeutics. The IQVIA (Durham, NC, USA) 2021 Digital Healthcare Survey (Fig. 1) indicates that in 2015, digital health applications (apps) focusing on exercise management, diet, and nutrition management represented 72% of digital healthcare’s objectives. By 2020, this figure had dropped to 54%. Conversely, the share of digital health apps designed for disease management and digital therapeutics in creased from 28% in 2015 to 47% in 2020 [1,2]. The significant growth in the bold navy-blue section of the graph, representing disease-specific health condition management, can be linked to the easing of regulations concerning digital therapeutics, which has spurred the active development of digital therapeutics software.
Digital therapeutics are defined by the digital therapeutics alliance, an international nonprofit organization, as evidencebased therapeutic interventions driven by high-quality software programs designed to prevent, manage, or treat medical disorders or diseases [1,3]. In the wake of coronavirus disease 2019, the U.S. Food and Drug Administration recognized the importance of digital therapeutics strategies for mental health and well-being during periods of quarantine and isolation. As a result, certain regulations were relaxed to expedite the distribution and use of digital therapeutics, thereby actively endorsing their importance [1,4]. Similarly, in South Korea, the value of digital therapeutics has been acknowledged, with relevant institutional advancements being undertaken primarily by health authorities and policy research organizations. In Korea, digital therapeutics are characterized as high-quality software that leverages digital technologies such as AI, VR, AR, apps, wearable devices, and others to provide evidence-based therapeutic interventions for the prevention, management, or treatment of medical disorders or diseases [5]. Digital therapeutics not only deliver therapeutic interventions directly to patients, but are also being incorporated into comprehensive healthcare services. Digital therapeutics offer additional functionalities such as mobile health services (mHealth), health information technology, medical devices (including devices, sensors, and wearables), and telemedicine, all within the framework of integrated medical services [6].
The fields where digital therapeutics development is most active include mental health, chronic diseases, and physical health. For mental health, digital therapeutics enable cognitive-behavioral therapy for conditions such as depression and anxiety, and they facilitate the development of tools for stress management and self-regulation enhancement [7]. In the realm of chronic diseases, digital therapeutics are primarily designed for diabetes and cardiovascular diseases. Examples of digital therapeutics in this domain include features for blood glucose monitoring and the integration of digital apps and smartwatches that track heart rate and blood pressure. Furthermore, by leveraging big data and AI, digital therapeutics provide lifestyle recommendations, help maintain healthy behaviors, and predict health outcomes, thereby becoming a significant element of digital healthcare content. In the area of physical health, development is underway for digital therapeutics that connect to bio-signal monitoring. These therapeutics support patient exercises and physical therapy, incorporating technologies such as VR and AR. Among the 3 areas of mental health, chronic diseases, and physical health, the surge in digital therapeutics for chronic diseases is primarily attributed to advancements in big data and AI technology. This surge is due in part to the fact that a significant portion of chronic disease patients are aging, and their hospital visit records, which accumulate over time, provide a rich source of data for preventive and therapeutic interventions. Additionally, chronic disease management can significantly benefit older adults by offering services that focus on lifestyle habit correction and prevention education. Moreover, the growing emphasis on developing digital therapeutics for chronic diseases is also driven by the capacity to analyze patient interactions with healthcare professionals and to predict patient conditions.
This study primarily focused on urinary dysfunction, a subset of chronic diseases, as the app area for digital therapeutics. The rationale behind this choice is threefold. First, although urinary dysfunction affects 40%–80% of the population as they age, as shown by survey statistics in Fig. 2, very few individuals receive lifelong urology care. According to previous research, 18% of women (506 individuals) and 37% of men (548 individuals) reported having received treatment [8,9]. This suggests a lack of provision of urological healthcare information and highlights the urgent need for pre-educational healthcare management to promote healthy living. Second, the National Health Insurance Service in South Korea reports that over 90% of bladder inflammation (cystitis) patients in Korea are women, yet there is a widespread misconception that it is a male-oriented condition. Consequently, female patients often seek obstetrics and gynecology care instead of urology care [10]. This misconception has led to cases where the diagnosis of bladder cancer in women is delayed during the evaluation of causes of hematuria, resulting in a higher cancer mortality rate than in men [11,12]. Therefore, it is essential to develop various digital therapeutics that enable predictive diagnosis, treatment, and management through self-assessment and life-logging data. Third, urinary dysfunction significantly reduces the quality of life for older adults [13]. Aging typically leads to a decline in almost all physiological functions. Despite the common occurrence of lower urinary tract symptoms with aging, many individuals often do not seek medical attention or treatment [14]. This can lead to fewer outings and limited participation in essential social activities, potentially contributing to depression among the elderly. Consequently, the provision of preventive and management-oriented services is becoming increasingly important [15].
To address these challenges and advance the field of digital therapeutics, we propose a content design model specifically for digital therapeutics that incorporates urinary dysfunction as its focus. This model aims to facilitate education, treatment, and prevention of chronic diseases.
RELATED RESEARCH
Definition of Digital Therapeutics
The key aspect of digital therapeutics is the requirement for tangible treatment outcomes and clinical evidence following their use. As depicted in Fig. 3, there is a clear distinction between digital therapeutics and digital healthcare: digital healthcare typically does not require clinical evidence, whereas digital therapeutics necessitate such evidence and must demonstrate treatment outcomes [16]. The researches of Amit et al. [17] and Yoo et al. [18] clarify that for medical technology to be classified as a digital therapeutic, its effectiveness must be substantiated with clinical evidence, including real-world data. Despite recent clinical trials providing substantial data for validation, digital therapeutics companies have yet to achieve significant penetration in mainstream healthcare [19]. This is attributed to 2 major barriers that are impeding the adoption and proliferation of digital therapeutics.
First, distinguishing between digital therapeutics and digital healthcare apps that focus on general health and wellness presents a challenge in the digital healthcare market. Second, national policies related to support in medical environments, such as insurance coverage and tax refunds, have not been firmly established. The bolded boxes in Fig. 3 delineate the roles of digital therapeutics across 3 stages of primary care, arranged into a 3P (pre-education, prediction/diagnosis/treatment, postmanagement) content model. This organization aims to clarify the areas in which digital therapeutics are distinct from general digital healthcare apps [20]. The critical need for digital therapeutics in future societies stems from their potential to enhance the traditional practice of primary care, previously limited to in-person hospital visits.
The first stage involves providing education and utilizing surveys, such as the Overactive Bladder Symptom Score (OABSS), to facilitate self-diagnosis and self-treatment before a patient visits a healthcare institution. The second stage encompasses a more accurate diagnosis for the initial assessment and treatment by digital therapeutics, enabling treatment anywhere, whether in a healthcare facility or through remote clinics. During this stage, healthcare institutions or physicians can make precise clinical diagnoses and treatment decisions based on data-driven information that corresponds to the patient’s symptoms. The third stage involves monitoring and tracking the patient’s response to the treatment prescribed by medical professionals.
In this study, we define 3 stages of digital therapeutics, distinguishing them from digital healthcare. Our focus is on the digitalization of patient data to facilitate easy access for individuals with chronic diseases. We also ensure that educational, therapeutic, and preventive content adheres to regulatory standards, enabling accurate treatment and prevention. Section 4 offers a detailed explanation of the prototype concerning urinary dysfunction in chronic diseases.
Analysis of Digital Therapeutics by Software Type
To acquire clinical evidence, it is necessary to review the technology employed in digital therapeutics. The sophisticated software technologies used in this field can be classified into 6 categories: (1) web/apps, (2) VR/AR, (3) games, (4) AI and big data, (5) brain-computer interfaces, and (6) biosensors. These technologies are applied in digital therapeutics for various therapeutic strategies, including cognitive-behavioral therapy, lifestyle habit modification, medication management, and neurorehabilitation.
Cognitive-behavioral therapy is effective in treating conditions such as insomnia, substance addiction, depression, and anxiety disorders. For patients with chronic diseases, including diabetes, cancer, hypertension, asthma, and chronic obstructive pulmonary disease, lifestyle habit modification and medication management have proven beneficial. Neurorehabilitation therapy is utilized to address brain-related injuries and conditions, such as dementia, autism, post-stroke disabilities, and attentiondeficit/hyperactivity disorder.
Table 1 summarizes the key technologies applied across various fields, categorized by therapeutic approach. Tables 2–4 provide an overview of the current status of digital therapeutics, with a focus on mental health and cognitive-behavioral therapy in Table 2, chronic disease management for lifestyle habit correction and medication management in Table 3, and brain-related injuries for neurorehabilitation therapy in Table 4. The organization of digital therapeutics products is informed by a reclassification of key applied technologies, therapeutic approaches, and software app technologies. This reclassification references reports from IQVIA (2021), Electronics and Telecommunications Research Institute (ETRI)’s technology policy report, and the Digital Therapeutics 2022 report for Korea [21].
Most digital therapeutics related to mental health depend significantly on web/app-based online counseling platforms (Table 2). These remote counseling platforms enable cognitive therapy that promotes the rectification and alteration of erroneous cognitions, thus aiding in the treatment of conditions such as insomnia prevention, substance addiction correction, and depression. The principal technologies employed are brain-computer interfaces, VR/AR, and AI.
Table 3 presents examples of the use of deep learning technology to collect, analyze, and learn from life-logging data collected via wearable devices. This data encompasses user activity, physique, body temperature, sleep patterns, among other metrics. Numerous companies have created platforms that link to medical institutions, enabling self-measurement through smart healthcare devices. These platforms aid in managing personal health records, encompassing prescriptions and check-up records, and provide options for linking with guardian accounts. The principal technologies applied include AI, big data, app/web development, and others.
Table 4 focuses on diseases caused by brain injuries. For dementia treatment, cognitive health programs or cognitive education programs are predominantly employed following memory assessments. For autism or physical disabilities, there is a shift toward the use of VR-based games linked to health devices, as well as the incorporation of VR content technology into video games [22,23].
Medical Decision-Making Technology
In 2011, the International Medical Device Regulations Forum established a distinction between 2 types of medical software devices: SiMD (software in a medical device), which is a combination of hardware and software, and software as a medical device (SaMD), which refers to standalone software. Digital therapeutics are classified as SaMD, denoting independent software constituting medical devices within the realm of information and communication technology. Notable examples of SaMD include computer-aided diagnosis and clinical decision support software (CDSS). These tools are utilized for disease diagnosis by providing information or aiding in clinical decision-making processes. The primary distinction between digital therapeutics and digital healthcare apps lies in the fact that digital therapeutics generate diagnostic predictions by integrating electronic medical records with various types of information.
CDSS supports healthcare professionals in making decisions by providing diagnostic assistance, treatment decision support, prescription guidance, information retrieval, medical image analysis, and risk alert information [24]. In South Korea, CDSS platforms have been developed and are in use at several hospitals, including Bundang Seoul National University Hospital, Severance Hospital, Samsung Seoul Hospital, and Asan Medical Center. However, their app is currently confined to certain areas. For these systems to be effective, accurate patient data collection is crucial. In chronic disease management, patients are subject to long-term medication regimens and ongoing observation, often utilizing the concept of activities of daily living for data gathering during each hospital visit. Nevertheless, the precision of the collected information can be affected by factors such as lengthy intervals between visits and memory limitations. For technologies like CDSS to become widely adopted, improvements in clinical information interoperability are essential. At present, the clinical element model (CEM), developed by Intermountain Health Care (IHC) in the United States, stands as the most recognized clinical information model. IHC has been refining the CEM to encompass the full range of clinical practice. This includes documenting a patient’s condition in electronic health records, symptoms for diagnosis, clinical and anatomical pathology, imaging studies, and prescriptions for medications [25,26]. Furthermore, for precise data collection, the development of medical devices is underway. These include wearable devices and smartphones, as well as Samsung and Apple smartwatches. Although not officially classified as medical devices, these smartwatches are used for collecting step data, as demonstrated by Three Labs Inc. in South Korea. They play a role in health management and digital healthcare by facilitating the use of patient-generated data. The integration of clinical information with lifelog-based data is progressively improving the precision and functionality of CDSS [27-29].
DIGITAL THERAPEUTIC CONTENT BASED ON THE UTILIZATION OF CHRONIC DISEASE HEALTH DATA
Evidence-Based Content Composition in Clinical Settings
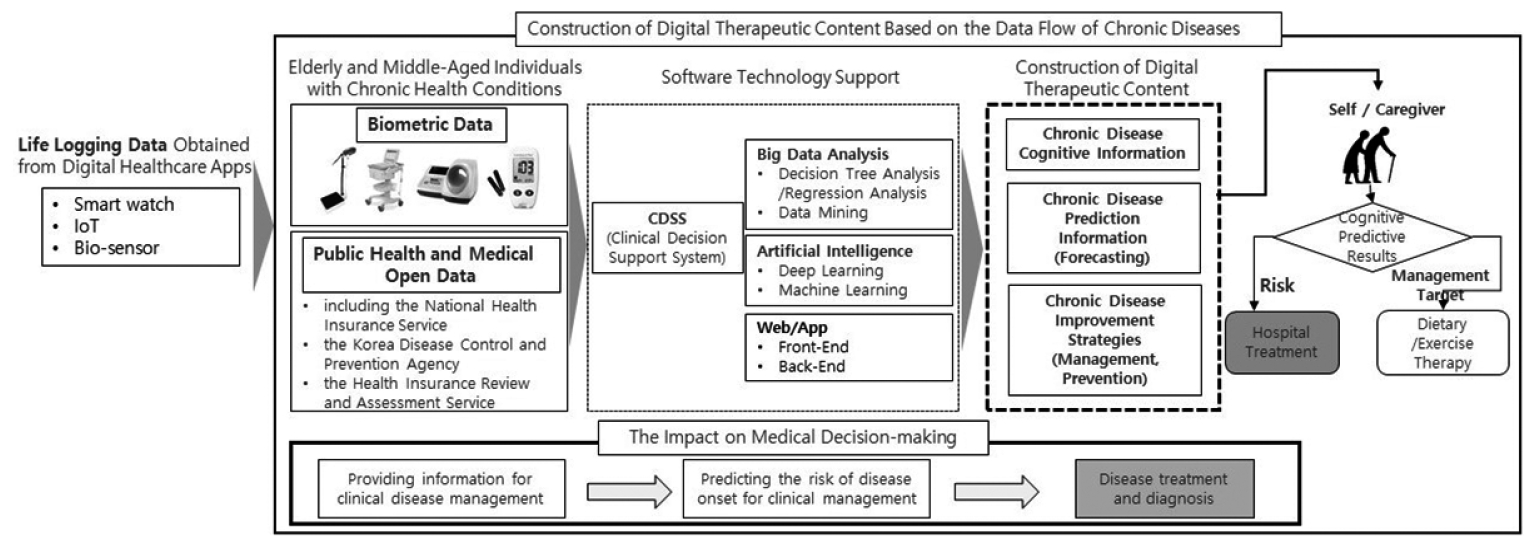
To establish digital therapeutics for chronic disease patients, it is essential to differentiate them from other software developed within the digital healthcare sector. This differentiation is primarily achieved through the acquisition of clinical evidence specific to chronic diseases. Most importantly, the collection of biometric data from medical devices, such as SaMD, is critical. SaMD is divided into 4 categories–types I, II, III, and IV–based on the significance of the information it provides. The ETRI report has utilized this classification to categorize the impact on medical decision-making that is informed by the information provided by SaMD, as detailed in Table 5 [6]. The impact on medical decision-making, as depicted in the lower thick box in Fig. 4, hinges on the accuracy of the data. This encompasses the provision of information for clinical disease management, including electrocardiography, weight, blood pressure, and blood glucose, as well as the prediction of disease onset risk. Following the prediction of disease onset risk, disease diagnosis and treatment ensue. In essence, the utility of digital therapeutics is increased as the accuracy of disease assessment based on data improves [30].
In this study, we analyzed biometric data from both elderly individuals and young adults with chronic disease findings, along with public health and medical data. We integrated these data sources with software technologies, such as big data and AI, within a CDSS. Consequently, the data was organized into 3 categories: chronic disease cognitive information, predictive information, and management/prevention information. These categories are part of the digital therapeutic content model, which is depicted within the dotted box in Fig. 4. The structured data is designed to be delivered to individuals or caregivers, supporting hospital treatment and dietary/exercise therapy as components of the digital therapeutic content model. A point of ambiguity arises in distinguishing between life-logging data and digital therapeutics. To address this, our study differentiated health data from life-logging data, classifying it exclusively as digital therapeutic data.
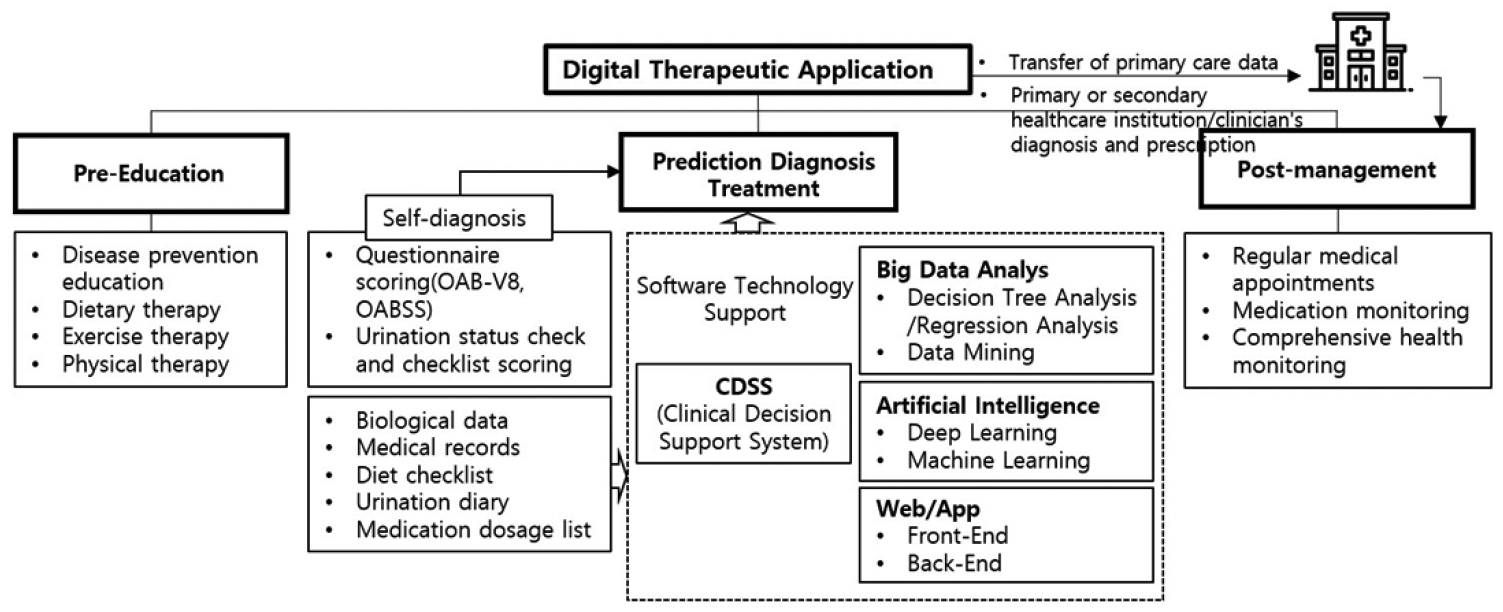
Evidence-Based Content
The life-logging data obtained from digital healthcare apps consist of activity data that users engage in to maintain their health; thus, clinical evidence is not typically required. Nevertheless, this data can be valuable for the postmanagement of chronic disease patients, as it enables the monitoring of patient or user activities. As depicted in Fig. 5, life-logging data have been intentionally designed for selective use in digital therapeutics when necessary. Fig. 3 outlines the content structure necessary for developing digital therapeutics software, which is organized into 3 distinct stages. In this study, to more clearly define the monitoring aspect– which was previously ambiguously connected to the roles of postmanagement and digital healthcare apps–a detailed design was implemented using the 3P model. This model is divided into 3 stages: (1) pre-education, (2) prediction/diagnosis/and treatment, and (3) postmanagement. It is referred to as the data-based digital therapeutic 3P content model, as highlighted by the dashed box in Fig. 5.
Individuals or caregivers who receive cognitive, predictive, and preventive information through technologies such as CDSS engage in treatment or management that encompasses dietary and exercise therapy as part of their care regimen. Subsequently, they transition to the postmanagement phase, which incorporates education and entails consistent monitoring. This monitoring includes features accessible not only via standard clinical systems but also through digital healthcare apps.
PROPOSAL OF APPLICATION CONTENT FOR PATIENTS WITH VOIDING DYSFUNCTION
The proposed 3P content structure was primarily designed to address aspects related to improving voiding dysfunction in chronic conditions. The app for voiding dysfunction was developed to maximize the effectiveness of digital therapeutics. It integrates postmanagement and pre-education stages as the central flow of content. Table 6 summarizes the content and functionality in accordance with the 3P structure.
Key Components of the Content
Based on the proposed 3P content model in Fig. 6, a prototype was developed to facilitate primary diagnosis of voiding dysfunction associated with chronic conditions. The initial stage involves pre-education, where preventive education and awareness enhancement are provided. In the subsequent stage, termed prediction/diagnosis/treatment, patients are given digital questionnaires, their voiding condition is assessed, a voiding diary is kept, digital urine volume and flow rate are measured, and postdiagnosis prescriptions are enabled. The final stage, postmanagement, incorporates features such as the automatic collection of physiological data, networking capabilities between hospitals and patients or their guardians, and access to other symptoms or health records, enabling patients or their guardians to effectively monitor the condition. The digital therapeutic app is designed to facilitate both self-diagnosis and primary diagnosis, enabling individuals to assess their own health. For digital therapeutics to be effective, it is crucial that they provide rapid and precise results during the primary diagnostic phase. Consequently, the app’s content is tailored for self-diagnosis and the monitoring of patients’ physiological information. It includes integration with clinical decision support platforms or comparable software technologies, enhancing treatment and ensuring that diagnoses are grounded in clinical evidence.
Enhancing the Efficiency of Digital Therapeutics
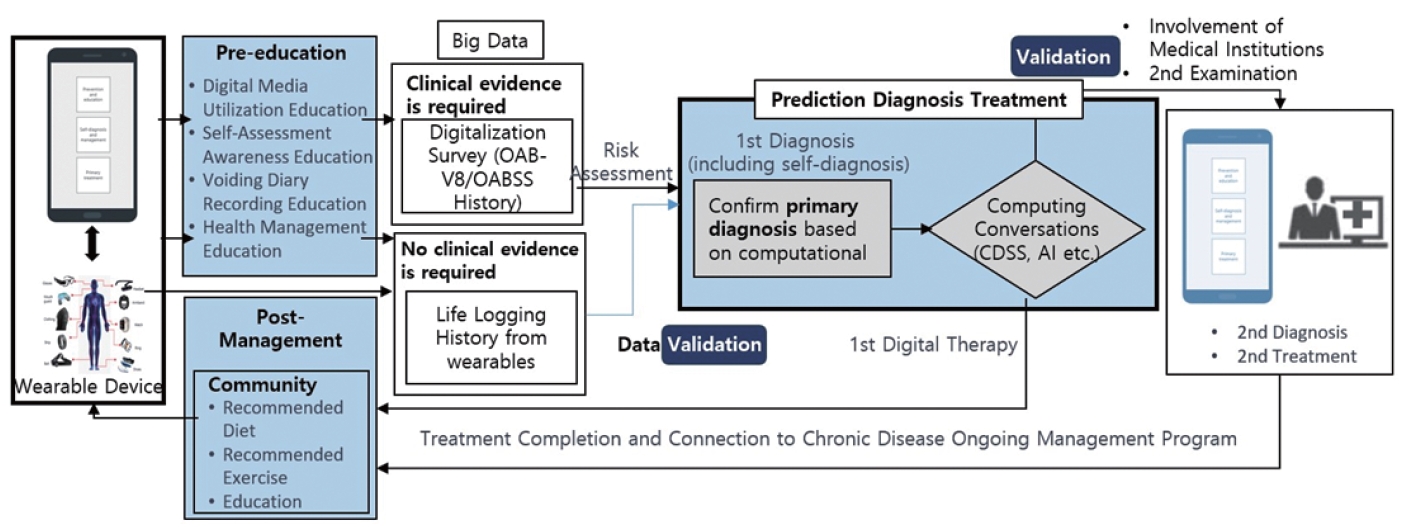
The most challenging aspect of designing the proposed 3P content model lies in differentiating between data that necessitate clinical evidence in digital therapeutics and data that do not require such evidence in digital healthcare. Within the flow structure of digital therapeutics, the “big data” box depicted in Fig. 7 is bifurcated into 2 categories to facilitate the verification process during the database construction phase. This structure is designed to distinguish between data that requires clinical evidence, such as overactive bladder-validated 8, OABSS, and voiding diaries collected in hospitals, and data derived from life-logging records, which do not require clinical evidence. In cases where data primarily sourced from digital healthcare app–typically gathered from wearable devices–do not require clinical evidence, the model incorporates a verification stage.
The effectiveness of digital therapeutics improves as the accuracy of the prediction/diagnosis/treatment phase increases. Fig. 7 highlights the importance of developing the digitalization stage, which includes self-diagnosis surveys and software technology, to enhance the precision of initial diagnoses. However, for an accurate diagnosis that involves the collection and validation of clinical evidence data, it is crucial to establish connections between secondary medical institutions and hospitals. In the final stage of postmanagement, which requires ongoing treatment and management over a prolonged period, a dedicated community is formed to concentrate on postmanagement and to integrate it with pre-education. This approach facilitates customized postmanagement that is adapted to different age groups. Within the community, particularly on social networking services, individuals with similar symptoms can interact and exchange information about their diets and exercise routines. The checklist features a voiding diary, a commonly utilized tool, which is therefore prominently placed in the main menu for user convenience.
Digital Prototype of the Application
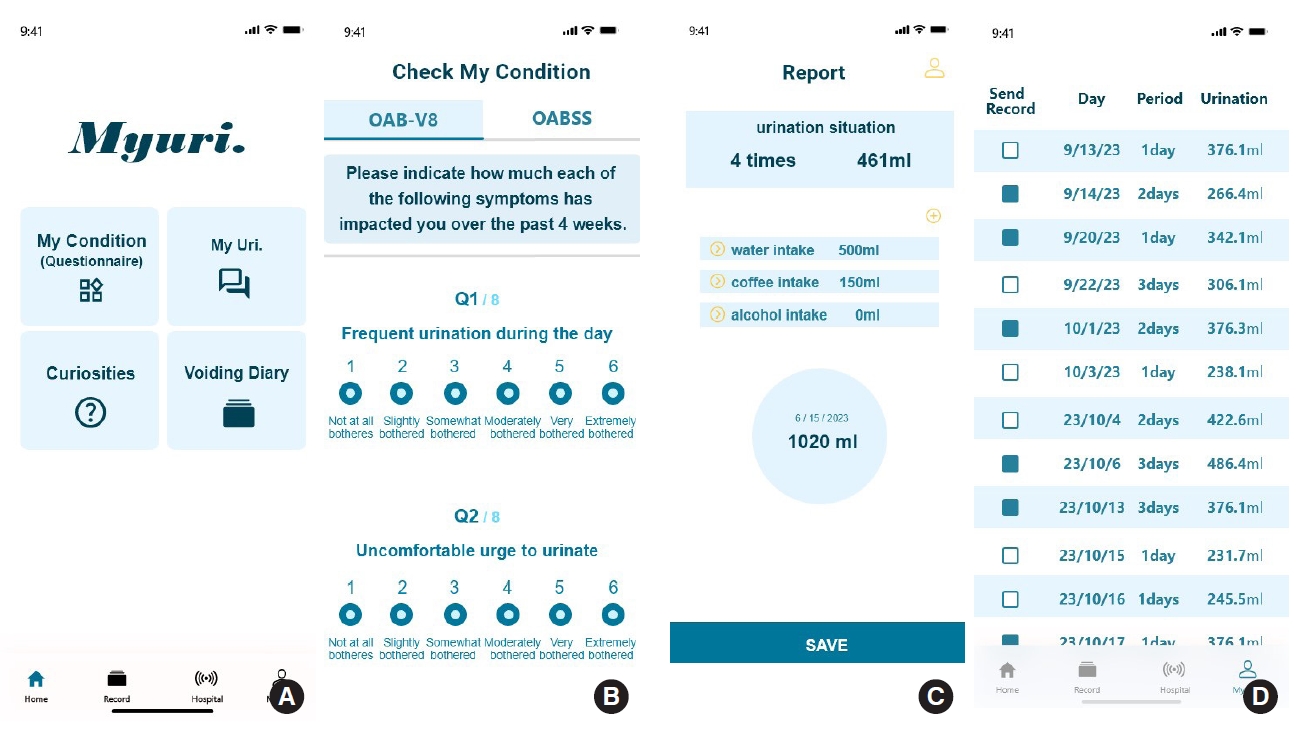
One of the essential components to be included in a digital therapeutic app is the capability for users to record their own disease symptoms using digital data [3]. Fig. 8A displays 4 tabs: self-diagnosis via questionnaire completion, a voiding diary, personal information sharing, and access to disease-related information. Upon selecting “my status (questionnaire),” users are directed to a screen where they can fill out the questionnaire, as depicted in Fig. 8B. At the screen’s bottom in Fig. 8C, options are available to save the entered information and transmit it to the hospital, which can be referenced in future medical treatment coordination. Selecting the “voiding diary” tab from the app’s main screen directs the user to a recording interface to log their voiding patterns. This section includes checkboxes for foods that may exacerbate an overactive bladder and options for recording the volume of voids from the previous day and the current day’s voiding status. In Fig. 8D, the “record” page, accessible via the top right corner, contains the “my page” icon, which allows users to review their long-term voiding history. For individuals diagnosed with voiding disorders at a hospital, an enhanced version of the app is available. This version offers more comprehensive voiding diary features, such as the ability to measure the volume and flow rate of urination. These advanced features are designed to sync with hospital records, providing a thorough approach to monitoring and managing voiding disorders. This integration supports realtime patient monitoring through a 24-hour remote voiding disorder monitoring system.
To ensure essential connectivity with healthcare institutions, the app can provide options where selecting one displays recommended diets, diet rankings, recommended exercises, prevention education-related videos and articles, and a list of nearby hospitals. As shown in Fig. 9, if the user chooses the ‘recommended exercises’ option among the choices related to primary treatment, they can experience content focusing on lifestyle correction and physical therapy for primary treatment. Additionally, users can easily view customized exercise videos recommended by the hospital after the doctor’s diagnosis within the app. Preventive exercises can be automatically recommended based on gender and age groups, including women, men, those in their 40s, 50s, 60s, and 70s and above. Furthermore, as age increases, video clips that can be watched and assist in exercising at home can automatically remove the background, zoom in on specific body parts, and emphasize detailed observation of body movements.
In this app, personalized services are tailored to specific age groups. The “video recommendations” feature prioritizes videos that focus on prevention and management, particularly for users in their 40s and 50s. It curates content in line with their preferences. Additionally, users have the option to share their exercise progress on social media platforms, fostering connections and interactions with peers in similar age brackets. For users in their 60s, the app provides a wealth of knowledge and educational content. If a patient is diagnosed with a voiding disorder, the app generates automatic warning messages and transmits voiding records to the hospital in the event of abnormal symptoms, based on the collected voiding data. For those aged 70 and above, the hospital icon on the initial screen of the app offers straightforward access to support information and educational resources.
CONCLUSION
This paper introduces a 3P content model designed to enhance the efficiency of digital therapeutics for patients with chronic diseases. The model aims to improve upon the traditional approach to primary diagnosis, which has typically limited digital therapeutics to in-hospital use. By providing pre-education, the model enables patients to engage in self-diagnosis and self-treatment prior to visiting healthcare facilities. Additionally, it facilitates the completion of digital surveys, such as the OABSS, outside of hospital settings, allowing patients to document more specific and detailed information on a daily basis. This capability ensures that medical institutions receive accurate patient data, which in turn supports healthcare providers in making timely and precise clinical diagnoses and treatment decisions. Moreover, for patients with chronic diseases, this feature is essential for ongoing management, as it allows for continuous monitoring and tracking to prevent relapse, highlighting its significance for the future of healthcare software.
The 3P (pre-education, prediction/diagnosis/treatment, postmanagement) model is based on the cyclical structure of clinical evidence-based disease symptom data for patients with chronic diseases. Within this cyclical structure of the 3P model, the ongoing generation and accumulation of patient physiological data are expected to become increasingly precise over time, thereby facilitating the advancement of personalized healthcare. Digital therapeutics and app emerging from digital healthcare are anticipated to play a pivotal role as the healthcare software of the future. These tools will be intimately integrated with medical institutions, providing convenience for both high-risk individuals and the general healthy population. This includes remote access to medical services, risk notifications, scheduling medical appointments, consultations, and obtaining prescriptions. Additionally, they will offer ease for caregivers of elderly patients and streamline insurance processes, as they are projected to interface with insurance providers. Nonetheless, the safety and reliability of digital therapeutics hinge on their compliance with usage scopes and regulations that are determined by the structural integrity of medical data. Consequently, research into the design of medical content, underpinned by cutting-edge technology, is of paramount importance.