INTRODUCTION
Neurogenic bladder (NB) due to spinal bifida is common in clinical practice. The upper urinary tract dilatation (UUTD) is a main cause of morbidity and mortality in children with NB [1]. Bladder compliance (BC) refers to the relationship between bladder volume and detrusor pressure and can be calculated from a cystometric pressure/volume curve. It is generally regarded as a measure of bladder stiffness or distensibility. A poor compliant bladder may increase the incidence of upper urinary tract infection and UUTD [2].
It has previously been reported that low BC is an independent predictor of UUTD [3]. The study of Kurzrock and Polse [4] revealed that BC value of <9 cm/cm H2O was an important risk factor for UUTD. Ghoniem et al. [5,6] confirmed the above viewpoints in their studies. Detrusor leak point pressure (DLPP) is also an important predictor of UUTD [5,7]. However, the literature on how to predict UUTD is still controversial. McGuire et al. [1] mentioned that approximately 70% of patients with NB and a DLPP value >40 cm H2O suffer from UUTD. Prakash et al. [7] reported that a DLPP value <40 cm H2O can also indicate UUTD, especially in the presence of vesicoureteral reflux (VUR) and an increased postvoided residual (PVR). Moreover, a recent study showed that a DLPP cutoff value of 20 cm H2O showed a higher sensitivity to predict UUTD than a cutoff value of 40 cm H2O [8]. Obviously, further studies should be performed to identify more accurate predictors of UUTD. With the advances of urodynamic study, it is possible to find more accurate urodynamic parameters to predict UUTD [9,10]. To our knowledge, there have been no reports on the relationships between BC and detrusor pressure or DLPP at different bladder filling stages and UUTD. Therefore, the purpose of this study is to evaluate the predictive value of a low BC, high detrusor pressure (△Pdet), and DLPP at different bladder filling stages for the diagnosis of UUTD in children with NB.
MATERIALS AND METHODS
A total of 158 children with NB who visited the First Affiliated Hospital of Zhengzhou University between 2018 and 2020 were included in this study, 39 of whom had UUTD. All patients were examined by ultrasound, intravenous urography, spinal magnetic resonance imaging, and video urodynamic study (VUDS). The patients were divided into 2 groups: group 1 (UUTD group) included 39 patients with bilateral hydronephrosis and VUR (range, 3–16 years), of whom 30 had spina bifida (including cases of occult and cystic spina bifida), 6 had cystic spina bifida that was repaired, and 3 had spina bifida injury. Group 2 (control group) included 119 patients without UUTD and VUR (range, 3–16 years), of whom 93 had spina bifida (including occult and cystic spina bifida), 18 had cystic spina bifida that was repaired, and 8 had spina bifida injury. Table 1 shows all the patients’ characteristics.
The results of VUDS were interpreted according to International Continence Society (ICS) and International Children’s Continence Society (ICCS) [11-14]. The urodynamic setting was a Laborie Urodynamic analyzer (Laborie Medical Technologies Inc., Mississauga, ON, Canada). A 6F double-lumen catheter was used to record the bladder pressure transurethrally. Room-temperature saline and dilute ioversol were perfused into the bladder at a rate of 10% of the expected bladder capacity (mL/min) [15]. The bladder filling endpoint was defined as the desire to void, a sensation of fullness or discomfort, or leakage around the catheter. The urodynamic parameters assessed included BC, △Pdet, the maximum flow rate, PVR, and maximum cystometric capacity (MCC). The DLPP is defined as the maximum detrusor pressure needed to overcome urethral resistance was also recorded. When no leakage was observed, DLPP was replaced with the maximum Pdet at the MCC [16]. The bladder filling phase was divided into 3 equal parts, namely, the early, middle, and end filling stages. During the cystometry and pressure-flow study, recording began from the pressure (Pdet0) when the bladder was empty (V0=0 mL) to the pressure (Pdet3) when the bladder was filled to the patient’s strong desire to urinate (V3). Then, we obtained the △V3 (△V3=V3–V0) and △Pdet3 (△Pdet3=Pdet3–Pdet0). In the same manner, we obtained △V1 and △V2 and △Pdet1 and △Pdet2 when the bladder volume increased to 1/3 and 2/3 of the MCC, respectively. According to the calculation formula of BC (BC=△V/△Pdet), we obtained the different BC values (BCx=△Vx/△Pdetx) in the early, middle, and end filling stages.
For the statistical analysis, t-test was used to determine the differences in BC and △Pdet in different filling stages between patients with NB with and without UUTD, and P<0.05 was regarded as statistically significant. The receiver operating characteristic (ROC) curves of BC and △Pdet in different filling stages were generated, the index on the point of tangency at the curve was identified, and the sensitivity (SEN) and specificity (SPE) were recorded. According to the formulas used to calculate the positive predictive value CPPV=1/[1+{1–SPE} {1–P}/ {SEN ×P}]) and negative predictive value (NPV =1/[1+{1– SEN}×P/{SPE–SPE×P}]), (P is the probability of UUTD in all pediatric patients with NB, and its value is approximately 40%) [17], the PPV and NPV were calculated. The accuracy of BC and △Pdet in different filling stages and DLPP to predict UUTD were analyzed by the area under the curve.
RESULTS
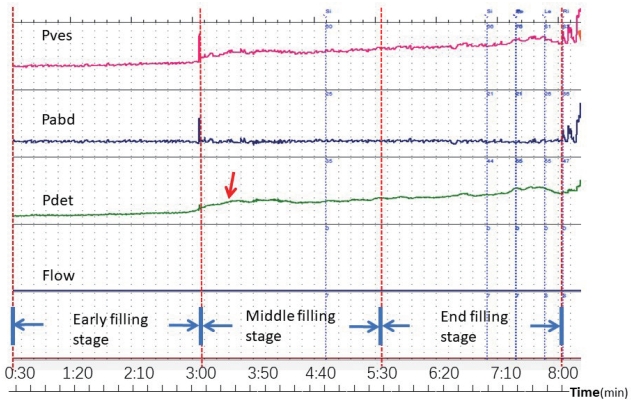
In the UUTD group (n=39), the pressure-volume (P-V) curves could be divided into 3 stages. The first stage (early filling stage) showed that the detrusor pressure increased slowly, the second stage (middle filling stage) revealed that the detrusor pressure increased quickly and then continued to increase slowly, and the end stage (end filling stage) showed that the detrusor pressure was at a stably high level (Fig. 1). In the middle and end filling stages, a positive correlation was found between the BC and UUTD as well as between an increase in △Pdet and a high prevalence of UUTD in all 3 filling stages (Table 1).
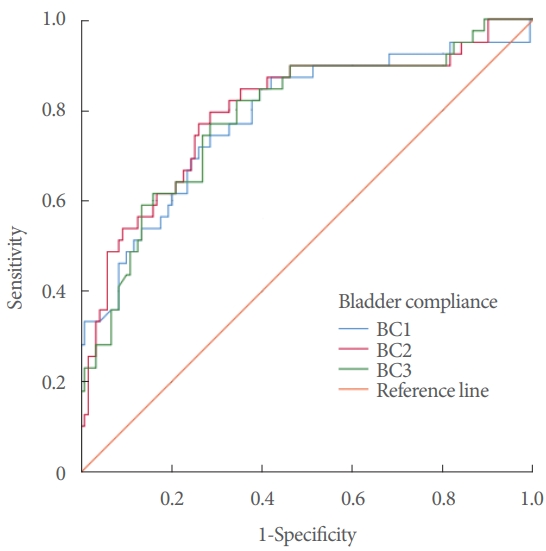
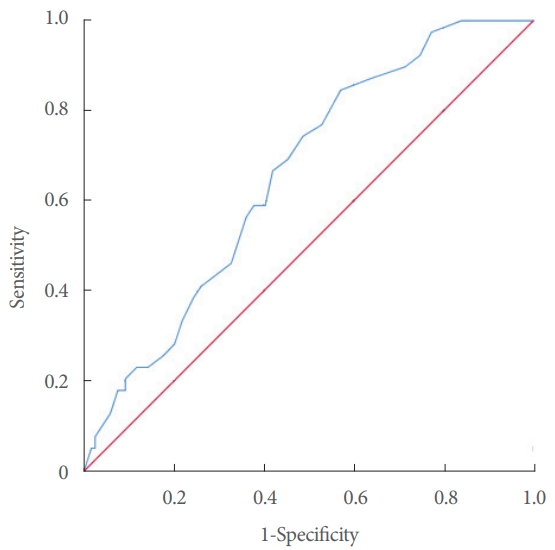
Patients with a BC value of <8 mL/cm H2O in the middle and end stages had a slightly higher SPE than those with a BC value of <9 mL/cm H2O in the end stage (72%, 73%, vs. 66%), but the SEN, PPV, and NPV were similar (Table 2, Fig. 2). The SEN of a △Pdet value of >8 cm H2O in the early filling stage, a △Pdet value of >20 cm H2O in the middle filling stage and a △Pdet value of >25 cm H2O in the end filling stage were significantly higher than that of a △Pdet value of >40 cm H2O in the end stage (82%, 85%, 85%, vs. 49%). A △Pdet value of >20 cm H2O in the middle filling stage was a better predictor of UUTD, with a PPV and NPV of 76% and 89%, respectively, according to the ROC curve (Table 3, Fig. 3). The DLPP of all children showed that a DLPP value of >20 cm H2O showed significance in predicting UUTD (Table 4, Fig. 4).
DISCUSSION
The detail relationship between bladder dysfunction and UUTD is still unclear and understanding its mechanism has always been an arduous task for urologists. Children with NB are more likely to develop VUR because of the immature mechanism of anti-reflux at the ureterovesical junction [3] or secondary to pathophysiological changes in the lower urinary tract, which contributes to UUTD. Urodynamic parameters are well known objective evidence to evaluate bladder function and it is important to investigate whether they and/or which one could be a more accurate parameter to predict UUTD during grow and mature of children with NB.
Normal micturition involves passive, low pressure bladder filling during the urine storage phase, while voiding requires the coordination of detrusor contraction and relaxation of the internal and external urinary sphincters. However, in pediatric patients with NB, high filling pressure of the bladder is caused by a pathological bladder wall, which can lead to UUTD. In NB, the inhibition of the pontine micturition center is weakened due to damage to the cortical and subcortical structures, which usually results in decreased bladder filling consciousness and low bladder capacity [18]. In addition, the pathophysiological changes in NB show individual variations. Therefore, it is not surprising that the values of low BC vary, ranging from 10 to 40 mL/cm H2O. Kaufman et al. [19] considered a ‘‘bladder storage pressure’’ of 40 cm H2O at typical filling capacity to be the pressure level for upper tract dilatation.
Two parameters, BC and △Pdet, have been reported in the literature to predict UUTD, and UUTD can be predicted according to the method by which the ICCS recommends calculating BC, but its accuracy is still not high. An ICS Teaching Module also showed that DLPP should not be used as the sole urodynamic parameter for predicting UUTD [20].
Kurzrock and Polse [4] and Ghoniem et al. [5] observed children with myelomeningocele or spina bifida in urodynamic studies and found that low BC was closely related to UUTD. A meta-analysis also suggested that low BC and high DLPP were major risk factors for UUTD [10]. Our results supported this finding, showing that the BC values of 3 filling stages in UUTD group were smaller than those in the no UUTD group significantly. Low BC could result in higher intravesical pressure than normal bladder and destroy the support of the detrusor muscle at the ureterovesical junction, resulting in the failure of the normal anti-reflux mechanism.
Kurzrock and Polse [4] reported that BC value of <9 mL/cm H2O was a better predictor of UUTD, with a poor PPV (52%). In our study, the PPV of BC value of <9 mL/cm H2O was only 60% and the PPV of BC value of <8 mL/cm H2O in the end filling stage was 65%. Neither were satisfactory for predicting UUTD. Therefore, it is not certain that the new indicator is more accurate than the classical indicator.
In addition, McGuire et al. [1] reported that a △Pdet value of >40 cm H2O was a risk factor for UUTD, with a PPV of 70%. In our study, the ROC curve revealed that the PPV of a △Pdet value of >40 cm H2O was 75%, but its SEN was only 49%, which was similar to the study of Teichman et al. [21]. Kurzrock and Polse [4] also indicated that a △Pdet value of <40 cm H2O can effectively prevent the development of UUTD (according to results after 11 years of follow-up). According to the ICCS definition of pediatric bladder function, a △Pdet value of ≤10 cm H2O could be considered essentially normal when the child’s bladder is filling to the expected capacity. Styles et al. [22] analyzed the relationship between UUTD and BC in 25 patients with chronic urine retention and found that there were statistically significant correlations between UUTD and both a high detrusor pressure in the end filling stage (Pdet >25 cm H2O) and a pressure increase during filling (△Pdet >15 cm H2O). The sensitivity was 93 and 100%, but the specificity was low (64% and 45%). Ozkan et al. [23] analyzed the urodynamic data of 35 patients with NB who did not undergo surgical treatment and found that a DLPP value of >75 cm H2O was a fairly high risk factor for UUTD. However, its PPV was not high (41%). In addition, the study of Çetinel et al. [24] showed similar findings. In our study, a DLPP value of >20 cm H2O showed significance in predicting UUTD but also had a low PPV (50%). Therefore, we know that a low BC, △Pdet, and high DLPP in the filling period are risk factors for UUTD in children with NB, but the parameters established in the literature are not satisfactory and cannot accurately predict UUTD [4,22,23].
Obviously, the identification of more accurate parameters or methods to predict UUTD is necessary. One method is to measure the value of BC in different filling stages. Early in 1989, Ghoniem et al. [6] divided BC into ‘‘initial’’ and ‘‘terminal’’ stages, when the initial slow rise in bladder pressure may turn into a rapid increase. By comparison, patients with good initial compliance did well clinically, while patients with poor initial compliance more commonly had VUR, deteriorated upper urinary tract morphology, and impaired renal function. He also found that a high DLPP (40 cm H2O or greater) and low BC (less than 10 mL/cm H2O) seem to be strong predictors of children at risk of UUTD [5].
In 1993, Gilmour et al. [25] analyzed the value of BC in different filling stages in 63 normal children and revealed that the minimum BC of normal bladder in normal children is 10 mL/cm H2O. He divided the filling process into 3 stages similar to ours but did not analyze them in detail by numerical values in children with NB. Present study showed detail numerical values of early filling stage, lower BC value is of little significance to UUTD. In this stage, the lower intravesical pressure achieved is due to the bladder is still empty. At the beginning of the middle filling stage, a further increase in bladder volume accompanied by a significant increase in intravesical pressure was observed, it might be due to the rate of stretch exceeds the rate of stress relaxation and then remains balanced as well as BC rises slowly. When the bladder continues to be filled in the end filling stage, the elasticity of the bladder gradually reaches its maximum elastic limit, and the pressure is not changed significantly anymore.
Therefore, we investigated BC in 3 different bladder filling stages and its relationship to UUTD and has found its good predictive value. The P-V curves in the majority (80%) of the patients with NB in our study showed a special characteristic; therefore, we divided the filling process into 3 stages. The first stage (early filling stage) showed that the detrusor pressure increased slowly, the second stage (middle filling stage) revealed that the detrusor pressure increased quickly and then continued to increase slowly, and the end stage (end filling stage) showed that the detrusor pressure was at a stably high level. This observation may be related to the increased stiffness caused by bladder fibrosis in children with NB. This phenomenon suggests that the △Pdet value in different filling stages could predict UUTD more accurately. Our study showed that a BC value of <10 mL/cm H2O was found in 76% of patients with NB in different filling stages. The accuracy of a BC value of <8 mL/cm H2O in the middle and end filling stages in predicting UUTD was slightly higher than that of a BC value of <9 mL/cm H2O, and a △Pdet value of >20 cm H2O in the middle filling stage had high accuracy, with an SEN of 85%, which was significantly higher than that of a △Pdet value of >40 cm H2O. The PPVs were similar (76% vs. 75%). The ability of a △Pdet value of >8 cm H2O to predict UUTD in the early filling stage was limited because its PPV was only 67%, which was lower than that of the study of McGuire et al. [1]. It is obvious that a △Pdet value of >20 cm H2O in the middle filling stage is a better predictor of UUTD. Overall, the ability of BC and △Pdet to predict UUTD in different filling stages is more accurate than reported in the above studies. This provided a possibility of finding an accurate time to perform intermittent catheterization to timely empty the bladder to prevent UUTD [26].
The relationships between other indicators, such as sex, disease course, urinary tract infection, bladder wall thickness, fecal incontinence, and UUTD, need to be further studied [2,7]. Research on the relationship between bladder capacity and UUTD is limited [19]. Çetinel et al. [24] reported that bladder capacity <200 mL was an independent risk factor for patients with spinal cord injury.
The main limitation of this study is that it is difficult to obtain accurate predictions with a small number of patients; the results of this retrospective study therefore need further verification. However, the findings of this study may provide new ideas for prospective studies with larger sample sizes in the future.
In conclusion, a low BC, a high detrusor pressure and an increased DLPP are good urodynamic parameters to predict UUTD, and these parameters reciprocally increase with the development of UUTD in children with NB. Both a △Pdet value of >20 cm H2O in the middle stage and of 25 cm H2O in the end filling stage are accurate indicators for predicting UUTD, with high sensitivity and specificity.