Daily Pad Usage Versus the International Consultation on Incontinence Questionnaire Short Form for Continence Assessment Following Radical Prostatectomy
Article information

Abstract
Purpose
Continence assessment is an essential component of follow-up after radical prostatectomy (RP). Several methods exist to assess the severity of urinary incontinence (UI). Our study examined the relationship and degree of agreement between International Consultation on Incontinence Questionnaire Short Form (ICIQ-SF) scores and the number of pads used in a 24-hour period in the assessment of UI following RP.
Methods
Continence was prospectively assessed in 746 men from a Spanish urology clinic 12 months after RP using the ICIQ-SF and pad usage. The relationship between ICIQ-SF scores and pad usage was assessed using Spearman rank correlation coefficients. The Jonckheere-Terpstra trend test was used to determine whether the ICIQ-SF score and the component question scores increased with increasing pad usage. The Bonferroni-corrected pairwise Wilcoxon rank-sum test was used to determine which pairs of pad usage levels differed. The weighted kappa was used to evaluate the agreement between pad usage levels and ICIQ-SF questions.
Results
The continence rate was 82% using the “no pad usage” definition of continence versus 78% using the definition of an ICIQ-SF score of 0 (P<0.001). Strong positive correlations were observed between the number of pads and the ICIQ-SF total and component question scores (rs>0.85, P<0.001). The ICIQ-SF total and component question scores increased significantly with increasing pad usage (P<0.001). The ICIQ-SF scores (P<0.018) for all pairs of pad usage levels (0, 1, 2, or 3 or more) differed significantly. The agreement between the ICIQ-SF leakage amount question and pad usage was very good (rs=0.861, P<0.001).
Conclusions
At 12 months post-RP, 24-hour pad usage was closely correlated with ICIQ-SF, although the continence rate differed depending on the definition used. Higher levels of pad usage were associated with higher questionnaire scores, more leakage, and poor quality of life (interference with everyday life).
INTRODUCTION
Urinary incontinence (UI) is a likely sequela of radical prostatectomy (RP) [1]. Wide variation exists in the terms used to define continence after RP, which affects the reported prevalence of UI [2]. The International Continence Society defined UI as “the complaint of any involuntary loss of urine” [3]. There is more agreement on using the time point of 12 months to define continence after surgery.
Several assessment methods have been developed to define and to measure the severity of UI, including pad weight testing protocols [1,4–6], patient self-report questionnaires [1,5,7], and documenting the number of pads used in 24 hours (pad usage) [1,5,8,9]: pad weight testing protocols offer an objective and quantitative measure of UI, and are considered the gold standard by some [6]. Questionnaires are a patient-reported tool that have ideally been validated and may show an impact on quality of life (QoL). The Short Form of the International Consultation on Incontinence Questionnaire (ICIQ-SF) is widely used in RP outcome studies. Using this instrument, a total score is derived from 3 questions; the first and second ask patients to subjectively evaluate the frequency and severity of their UI symptoms respectively, and the third evaluates condition-specific QoL, in which the interference of UI with everyday life is evaluated using a scale from 0 (not at all) to 10 (a great deal) [10]. The number of pads used per day is an easy way for patients to report their experiences, and is an accessible method for assessing severity, for which reason it is the most frequently used tool to assess UI after RP [1,11].
The aim of this study was to comprehensively examine the relationship and degree of agreement between daily pad usage and the ICIQ-SF total and question scores.
MATERIALS AND METHODS
Following institutional ethical approval, consecutive consenting patients who underwent RP for clinically localised or locally advanced prostate cancer were recruited between September 2002 and December 2011. Patients who underwent salvage RP after radiation therapy were excluded. Patient characteristics including surgical and pathological factors were recorded. Continence status was assessed at 12 months following surgery using (1) the total score of the Spanish version of the ICIQ-SF [12] and its component questions and (2) the patient-reported number of pads used within a 24-hour period (pad usage). Information was gathered on the type of pad (compress or diaper) and degree of absorption: level 1, 2, or 3 for compress pads and dayand night-time use diapers, respectively. Pad usage was divided into 4 levels: 0, 1, 2, and 3 or more pads, due to the small number of patients who used more than 3 pads per day.
Statistical Analysis
Means and standard deviations or medians and interquartile ranges (IQR) were used to describe continuous variables. Categorical variables were summarised using counts with percentages or proportions. The McNemar test was used to determine differences in continence according to the definition used. Spearman rank correlation coefficients were used to measure the strength of the relationship between pad usage and ICIQ-SF scores. The Jonckheere-Terpstra trend test [13] was used to determine whether the ICIQ-SF question and overall scores increased with increasing levels of pad usage (0, 1, 2, or 3 or more). If the Jonckheere-Terpstra test indicated significance, the Bonferroni-corrected pairwise Wilcoxon rank-sum test was used to determine which pairs of pad usage levels (0, 1, 2, or 3 or more) had significantly different ICIQ-SF scores. These methods were used due to the nonnormality of the scores. Treating the data as categorical, the Fleiss-Cohen weighted kappa statistic [14] was used to determine the agreement between pad usage levels and the related ICIQ-SF question regarding leakage amount (question 2). Kappa values (κ) were interpreted as poor for κ <0.20, fair for 0.21 <κ <0.40, moderate for 0.41 <κ <0.60, good for 0.61 <κ <0.80, and very good for 0.81<κ<1.00, as described by Altman [15]. To compare pads and ICIQ scores by type of pad, we performed the Student t-test. R statistical software ver. 3.5.2 (R Foundation for Statistical Computing, Vienna, Austria) and a 5% significance level were used for all analyses.
RESULTS
In total, 787 consecutive patients underwent RP for clinically localised or locally advanced prostate cancer between September 2002 and December 2011. Forty-one patients were excluded because they had undergone salvage RP or were lost to follow-up. A total of 746 consenting patients were included in the analysis. The demographic, clinical, and surgical characteristics of patients are presented in Table 1.

Demographic, clinical, and surgical characteristics of the participants (n=746)
The continence rate using the “no pad” definition of continence (82.3%) was significantly higher than the rate calculated when continence was defined as an ICIQ-SF total score of 0 (78%) (P<0.001). Table 2 shows information on patients divided first by their questionnaire answers and then by pad usage. Question 4 collected information on the situations in which patients experienced leakage, and it should be noted that some patients reported experiencing leakage in more than one situation. Overall, 14 (8.5%) reported urgency before UI and 109 (66.4%) reported stress-based UI.

Characteristics of incontinence
The daily number of pads used by the participants was as follows: 1 pad by 74 men (9.9%), 2 pads, 31 (4.2%); and 3 or more pads, 27 (3.6%). The median (IQR) ICIQ-SF total and question scores for each level of pad usage are presented in Table 3.
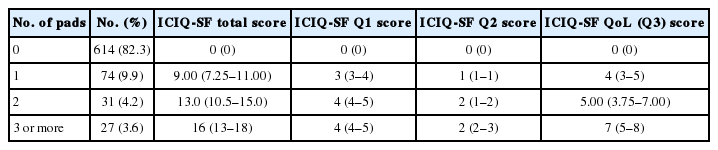
Pad usage count (%) and median (IQR) ICIQ-SF scores
Strong positive Spearman correlation coefficients were observed between pad usage and the ICIQ-SF total score (0.865, P<0.001), ICIQ-SF question 1 score (0.861, P<0.001), ICIQ-SF question 2 score (0.861, P<0.001) and ICIQ-SF QoL question 3 score (0.853, P<0.001).
The ICIQ-SF total and component question scores increased significantly with increasing levels of pad usage (P<0.001). The ICIQ-SF total and QoL question 3 scores differed significantly between all pairs of pad usage levels (0, 1, 2, or 3 or more pads) (P≤0.018 and P≤0.025, respectively). For the remaining questions, the ICIQ-SF question 1 and 2 scores differed significantly (P<0.001) between all pairs of pad usage levels, except for the use of 2 pads versus 3 or more pads (Q1: P=1.000 and Q2: P=0.071, respectively).
Table 4 shows a cross-tabulation of pad usage levels and the categories of ICIQ-SF question 2 (small, moderate, or large amounts of leakage).

Count of pad usage level versus ICIQ-SF Q2 categories (n=746)
We hypothesized that if a patient complained of more leakage, the patient would use more pads each day, and then we measured the level of agreement between these parameters. There was very good agreement between levels of pad usage and the ICIQ-SF question 2 categories (κ =0.83; 95% confidence interval, 0.78–0.88). Most patients (655 of 746, 87.8%) showed agreement between the leakage amount and pad usage level. A few patients (on the nondiagonal parts of Table 4) wore more or fewer pads than we might expect given their leakage level.
Finally, we compared the number of pads that patients needed according to the type of pad (compress vs. diaper: 1.72±1.19 vs. 2.17 ±1.23; P =0.78). We then compared ICIQ-SF scores (compress vs. diaper: 10.74±3.7 vs. 13.9±3.46; P=0.000); and finally question 3 about QoL (compress vs. diaper: 4.41±2.24 vs. 5.4±2.0; P=0.033).
DISCUSSION
In a large sample of men (n=746), the reported continence rate using definitions of no pad usage or an ICIQ-SF total score of 0 was similar to those reported in some previous investigations [16,17], but higher than has been reported in others [5,18]. We must emphasize that prevalence can change considerably depending on the definition.
The number of pads used per day (in a 24-hour period) is the most frequent way to report incontinence in studies of RP outcomes, as it is easy for patients to report [19] and reflects materials that they use in their everyday lives. It is also sufficient to assess daily routines [20], and a previous study found that patients accurately described the number, size, and degree of wetness of pads [19]. Studies have reported significantly worse health-related QoL in patients using 1 pad than in those who were pad-free [21,22]. Pad usage is also a component question included in the Expanded Prostate Cancer Index Composite [23,24].
Pad weight protocols result in a measured variable [19], which better shows the severity of incontinence in a way that is especially valuable when offering a surgical device and is useful as an objective measurement of urine loss in clinical trials [20]. However, these protocols require a high level of patient engagement, logistical collection difficulties limit their daily use [20], and the results vary depending on daily activity level and fluid intake [25].
However, the number of pads used per day has shown issues with unreliability as a measure due to variations in volume and has demonstrated weaker correlations in comparison with pad weight tests in both men and women [26]. As such, pad usage has been supported by some [1] and challenged by others [5,16,26,27].
Questionnaires offer validity, reliability, and responsiveness to change, as exemplified by the ICIQ-SF, which is a patient self-reported tool that has advantages and disadvantages [1,10]. It has been validated against the 24-hour pad test and more invasive urodynamic assessments [7,27,28], and has been used in clinical trials and observational studies [29].
Due to the multifactorial origin of UI, there is a high-level division of most patients depending on whether they have reduced bladder capacity and/or reduction of sphincteric activity and urethral closure pressure. This should be taken into account before planning surgical treatment, but it is not routinely reported by groups that study outcomes after RP. We identified that 66.4% of patients experienced stress-based UI and 8.5% experienced UI due to urgency; thus, the bladder should not be forgotten as a factor, even if it has no impact on the initial diagnosis [30]. It is especially important to consider treatment with oral medications or surgical treatment such as a male sling or an artificial urinary sphincter [31]; furthermore, urodynamic studies may be required, and it may also be necessary to perform cystoscopy to discard anastomosis strictures. The success of surgical treatment was also measured by a reduction in pad usage [32].
We found that increasing pad usage was closely correlated with higher ICIQ-SF total scores and with each question (on urinary leakage frequency, severity, and QoL scores). No other study has investigated this issue.
We did not find significant differences in the number of pads used according to the type of pad, but we did find such a difference in questionnaire scores (almost 3 points), which we believe is quite relevant. We compared the QoL results by the type of pad used, and found a difference of 1 point, but we do not consider this difference to be clinically relevant. Furthermore, other authors have reported that the number of pads used had a significant effect on QoL and psychosocial function [33,34].
We did not conduct a more in-depth analysis of the type of pad used due to the risk of bias in analyses of smaller groups.
Despite the large sample, our investigation has some limitations. The patient cohort was drawn from a single centre. To perform a comprehensive assessment of correlations between tools, a pad weight testing protocol should be included to obtain more evidence. Furthermore, we only assessed patients at a single time point in their recovery following RP, and therefore measured the prevalence of UI instead of the time until the recovery of continence. Our results show that both tools were correlated, but the ICIQ-SF was a more sensitive tool; moreover, 35 patients (4.6%) reported leakage but did not wear any pads, which demonstrates the complexity of the disease. Pad usage and questionnaires offer useful information, but neither substitutes for the other.
In conclusion, the number of pads used in 24 hours was significantly correlated with ICIQ-SF scores in men at 12 months following RP. The questionnaire was more sensitive, as different continence rates were found in our series according to the definition used. Increased pad usage was associated with higher questionnaire scores, a higher amount of leakage, and poor QoL (interference with everyday life).
Notes
Research Ethics
This study was approved by the ethics committee of Clinica Universidad de Navarra within the Applied Medical Research’s first author dissertation.
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTION STATEMENT
·Conceptualization: SFM, JER, AT
·Formal Analysis: PLG, SFM
·Investigation: JIP, David Rosell, AT
·Methodology: JER, FDC
·Project Administration: SFM, JER
·Writing – Original Draft: SFM, PLG, MIP
·Writing – Review & Editing: AT