In female patients who are refractory to conservative treatments such as pelvic muscle exercise or presented with severe symptoms, surgical treatment is the most effective for the treatment of female stress urinary incontinence (SUI). Its success rate including a complete cure and an improvement of the symptoms has been reported to be approximately 70 to 90% and this corresponds to a relatively higher value [1]. The recent trends in the surgical treatment of SUI are that various types of non-invasive treatment regimens such as tension-free vaginal tape (TVT), transobturator tape (TOT), intravaginal sling plasty and suprapubic arc sling based on a synthetic tape (polypropylene monofilament or multifilament) have been introduced. Meanwhile, the number of patients who receive the treatment for SUI has also been increased. These surgical treatment regimens based on a synthetic tape are relatively non-invasive, simpler in technique. Besides, they have also been reported to have an excellent profile of treatment effect and treatment success. As the time elapsed, however, complications associated with a synthetic tape have been reported to occur. Besides, there are also some cases in which the fatal complications occurred.
We experienced a 39-year-old woman who had an anterior urethral erosion developed due to a synthetic tape and cellulitis occurring following the surgical treatment of SUI as a midurethral sling procedure. To our knowledge, this was not seen in a prior publication. Here, we report our case with a review of literatures.
CASE REPORT
A 39-year-old woman had received the pharmacological treatments for a 1-year-history of symptoms such as recurrent SUI, vaginal discharge, perineal pain, and vaginal odor. The patient was referred to us from the local obstetrics & gynecology clinics following the diagnosis of recurrent Bartholin's abscess and recurrent SUI.
On past history, the patient had undergone surgery 13 years before for the management of SUI. We could not know the name and type of that operation. Due to the recurrence of incontinence symptom, the patient had also received TOT procedure (Tension Free Obturator Tape, Dowmedics Co., Wonju, Korea) three years ago. TOT is a macroporous, polypropylene, monofilament type tape. Besides, the patient had also received hemorrhoid surgery one year before. Thus, she complained of above-mentioned symptoms at 2 years later after TOT procedure. Under impression of Bartholin's abscess, the patient underwent Bartholin gland duct incision and drainage at that clinic. But there were no other notable systemic findings on past history.
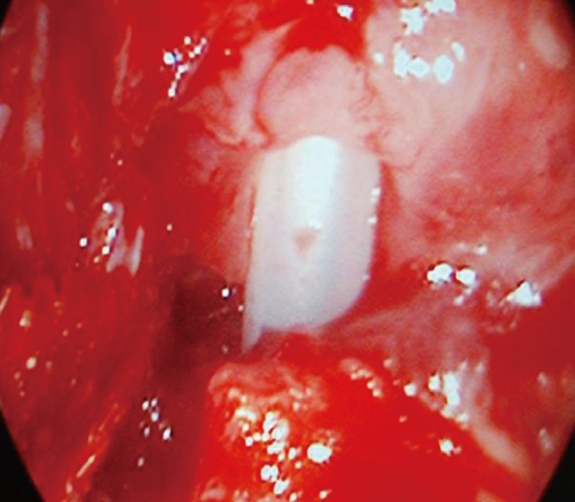
On admission in our urologic department, the patient had a good profile of nutritional status and systemic one. There were also normal findings in vital signs such as blood pressure, heart rate and body temperature. On physical examination, the patient had a tape suspected TOT mesh protruded to the anterior vaginal wall and urethral erosion (Fig. 1). Besides, there was a scar left following an incision and a drainage of Bartholin's gland on the left side of medial vaginal wall.
When an indwelling urethral catheter was inserted, the catheter was palpated and then observed to the inside of dissected urethra within the vagina on the posterior side of a tape which was exposed to the anterior vaginal wall. Around the vagina to which a catheter was exposed, there were inflammatory tissue and cellulitis (Fig. 2). The patient had severe vaginal odor and complained of the tenderness on vaginal palpation.
Firstly, the patient underwent a urine culture test and a peri-urethral culture in vagina and then had Pseudomonas aeruginosa identified. This was followed by a 2-week antibiotic treatment and wound disinfection. The patient had a decreased vaginal discharge and negative results to a urine culture test and a wound culture test. Thus, surgery was performed under spinal anesthesia, for which the patient was laid in a lithotomy position. Then, following the removal of a tape for SUI, a cystoscope was inserted via a vagina. It was thus confirmed that more than half of the urethral tissue were lost due to the erosion and the peri-urethral tissue was necrotized tissue around the urethra were confirmed. Following the sufficient removal of dissected para-urethral tissue, an end-to-end anastomosis was performed for the dissected urethra using the adjacent tissue (Figs. 3, 4). On postoperative day 8, the patient had a catheter removed. On postoperative day 9, the uroflowmetry study showed the maximal urinary flow rate 39.9 mL/sec, the voiding amount 398 mL and the amount of residual urine after voiding 17 mL. During a 12-month postoperative period, the patient received an outpatient follow-up. Thereafter, the patient had no notable findings on physical examination. Besides, the patient presented with no complications such as voiding difficulty or recurrent incontinence.
DISCUSSION
Surgical treatment methods using a synthetic tape for SUI, such as TOT and TVT, may produce postoperative complications and these include bladder puncture, hematoma, urgency, urinary retension, urinary tract infection, wound infection, vaginal erosion, vascular injury, and bowel injury. Of various complications, as the time elapses, the incidence of complications has been increased in association with a synthetic tape which is used for the procedure.
It has been reported that vaginal erosion and infections occur at an incidence of approximately 1% [2]. In 1997, the American Urological Association incontinence clinical panel performed a meta-analysis, according to which the incidence of vaginal mucosal erosion due to a synthetic substance was reported to be 0.7% [3]. Shah et al. [4] also reported that the incidence of vaginal mucosal erosion due to a synthetic substance during a sling procedure with a polypropylene mesh was 6.2 to 7.2%. And Karram et al. [5] reported that the incidence of vaginal erosion following incontience surgery with a synthetic tape reached a value of 0.2 to 22%. Novara et al. [6] reported that the incidence of vaginal erosion was 0.4 to 3.8% following TVT surgery according to a review of literatures which have been published during the 2000's. In Korea, Kim et al. [7] have recently reported that the incidence of vaginal erosion following a sling procedure was 1.4%.
It has been reported that there are rare cases of complications which should be surgically corrected following a sling procedure [8]. Vaginal erosion is a rare complication, and it occurs due to an inappropriate suture of the surgical sites following incontinence surgery, wound infection, delayed wound healing and foreign body reactions. And it is known as a risk factor in obese patients, diabetic ones and immunocompromised ones [5]. It is known that the removal of a sling tape is important for the treatment of vaginal erosion following a sling procedure. It can commonly be encountered, however, that patients are not actually in need of the treatment due to economic and psychological reasons. In these cases, however, there is a possibility that symptoms might be aggravated due to the delayed treatment. This leads to the speculation that the active treatment should be recommended.
In the current case, there was a past history of pelvic surgery which may be a risk factor. And, following the exposure of a synthetic tape due to vaginal erosion, the wound was aggravated due to the continuous infections and Bartholin's abscess. This might be responsible for the occurrence of urethral erosion and dissection. Besides, the vaginal damage due to a repeated incontinence surgery and the foreign body reactions occurring during wound healing might also be responsible for the occurrence of urethral erosion and dissection.
To prevent the possible occurrence of postoperative complications, the possibility for the intraoperative contamination of surgical wound should be minimized. In cases of postoperative complications such as vaginal erosion and infections, a complete removal of the infected tissue and a tape as well as the administration of sufficient antibiotics would be mandatory. Although a midurethral sling procedure, which is performed for patients with SUI, is a relatively simple method that causes a lesser extent of complications, there is a possibility that complications might occur and then affect the clinical course of patients as shown in this case. This may also lead to the occurrence of other complications. Accordingly, a regular follow-up observation might be mandatory for the possible occurrence of postoperative complications.