Correlation Between Nitric Oxide and Urodynamics in Men With Bladder Outlet Obstruction
Article information

Abstract
Purpose
To investigate the correlation between nitric oxide (NO) and urodynamics in men with bladder outlet obstruction (BOO) by analyzing nitric oxide synthase (NOS) in the urothelium.
Methods
We prospectively enrolled 25 men who planned to undergo surgical treatment for benign prostatic obstruction and identified as BOO in the preoperative urodynamics. Bladder tissue was taken during surgical prostate resection. Expressions of endothelial NOS (eNOS), inducible NOS (iNOS), and neuronal NOS (nNOS) in the urothelium were analyzed, and their correlation with urodynamic parameters was also assessed in all patients. We also compared the expressions of eNOS, iNOS, and nNOS between BOO with detrusor underactivity (DU) group and BOO without DU group.
Results
In all patients, the level of eNOS positively correlated with maximal flow rate and with maximum cystometric capacity (MCC). The level of iNOS positively correlated with MCC. nNOS levels were positively correlated with detrusor pressure at maximal flow and with bladder contractility index in all patients. The level of eNOS, iNOS, and nNOS did not significantly differ between BOO without DU group and BOO with DU group.
Conclusions
This study suggests that NO was correlated with bladder dysfunction in men with BOO. Particularly, nNOS may reflect the change in detrusor function.
INTRODUCTION
Bladder outlet obstruction (BOO), which is characterized by reduced uroflow rate and increased residual urine volume despite increased detrusor pressure, can cause morphological and functional changes to the bladder, resulting in either an underactive bladder or an overactive bladder [1,2]. Patients with benign prostatic obstruction (BPO), which is one of the most common causes of BOO in men, experience not only voiding symptoms but also storage symptoms that can have a considerable negative impact on the quality of life. Moreover, BOO-induced bladder function changes can be related to the lack of improvements in subjective or objective findings even after surgical treatment for BPO [3]. At present, the most reliable diagnostic method for bladder changes due to BOO is urodynamics. However, this method has some limitations, such as being invasive and time consuming. Although urodynamics is the only investigation to explore detrusor underactivity (DU) or detrusor overactivity (DO), the diagnostic criteria of them are various and uncertain yet. Thus, the development of new biomarkers is needed for a less invasive and more accurate diagnosis of bladder functional changes. For new biomarkers to be applied to the patients with lower urinary tract symptoms, they must be able to diagnose the patient’s condition, reflecting the results of the current urodynamics.
Pathophysiological changes in the urothelium induced by BOO are receiving attention as a new biomarker for diagnosing bladder dysfunction [4]. The urothelium acts as a sensor of various stimuli and is able to release various neurotransmitters that would modulate detrusor contraction and relaxation [5]. Nitric oxide (NO), which is catalyzed by 3 different isoforms of NO synthase (NOS) (i.e., endothelial NOS [eNOS], inducible NOS [iNOS], and neuronal NOS [nNOS]), could act as a neurotransmitter in the urothelium and influence the bladder function. Several previous animal studies have shown that the NOS isoforms show changes depending on the status of bladder function, such as an increase in nNOS and eNOS expression in DO associated with BOO [6] or a decrease in eNOS expression in BOO, which is responsible for bladder dysfunction [7]. However, the differences in the expression levels of NOS isoforms in the urothelium depending on bladder function remain unclear. The role of urothelial NO in bladder dysfunction has been mainly investigated in animal studies, and only a few human studies have been performed. In the present study, we aimed to investigate the correlation between NO and urodynamic parameters in men with BPO through the analysis of NOS isoforms in the urothelium.
MATERIALS AND METHODS
Study Population and Design
The study participants were a new set of 25 men aged 50–75 years old who were scheduled for surgical treatment for BPO, such as transurethral resection of the prostate or holmium laser enucleation of the prostate, and underwent preoperative urodynamics. Urodynamics was conducted in accordance with the Good Urodynamic Practice standards recommended by the International Continence Society [8]. Patients who were diagnosed with prostate cancer before or after surgery for BPO, and those with histories of prostatic and/or urethral surgery, acute urinary tract infection or indwelling bladder catheterization within 1month, interstitial cystitis/bladder pain syndrome, and lower urinary tract malignancy were excluded.
Bladder specimens were obtained using 3 cold cup biopsy from the posterior bladder wall during bladder filling of 150–200 mL just before surgery. The specimens were frozen in liquid nitrogen until use in the analysis. The expression of eNOS, iNOS, and nNOS in the urothelium was evaluated using enzyme-linked immunosorbent assay (ELISA) and immunofluorescence staining. We investigated the correlations between the expression of each NOS isoform in the urothelium and the urodynamic parameters. We also compared the expression levels of each NOS isoform between patients with DU and those without DU. DU was defined as a bladder contractility index (BCI) of <100 in urodynamics.
ELISA and Immunofluorescence Staining for NOS Isoforms
ELISA and immunofluorescence staining for the NOS isoforms were performed as described in our previous study [9]. The specimens were rinsed with 1 × phosphate-buffered saline (PBS), homogenized in 500 μL of 1× PBS, and stored overnight at -20°C. After 2 freeze-thaw cycles were conducted, the homogenates were centrifuged and the supernatant was removed. The levels of eNOS and iNOS in the specimens were measured, according to the manufacturer’s instructions, using a human eNOS ELISA kit and a human iNOS ELISA kit (Cusabio Biotech LLC, Houston, TX, USA). The nNOS levels in the samples were measured using a human nNOS ELISA kit (MyBioSource Inc., San Diego, CA, USA). The optical density of each well was determined within 5 minutes using a microplate reader (VersaMax, Molecular Devices LLC, San Jose, CA, USA) set to 450 nm and 540 nm.
For immunofluorescence analysis, we used antibodies against eNOS (1:100 dilution; Abcam Ltd., Cambridge, UK), nNOS (1:200; Abcam Ltd., UK), and iNOS (1:200; Thermo Fisher Scientific, Waltham, MA, USA). The slides were rinsed and then incubated with the secondary antibody (Alexa Fluor 488-labeled goat anti-rabbit IgG, 1:300; Molecular Probes, Eugene, OR, USA) at room temperature for 2 hours. After rinsing the samples again, the slides were stained with 4',6-diamidino-2-phenylindole (Vector Laboratories, Burlingame, CA, USA), and examined using a fluorescence microscope (BX50; Olympus, Tokyo, Japan).
Statistical Analysis
The sample size, calculated by the expected mean difference of 0.01, the standard deviation of 0.008, beta error of 0.2, and alpha error of 0.05, was planned to recruit 15 patients per county and a total of 30 patients, taking into account 10% dropout rates per county. All data are reported as means with standard error of means. The mean values were statistically compared using the Mann-Whitney U-test for all continuous variables and Fisher exact test for categorical variables. We analyzed the correlations between each NOS isoform in the urothelium and the urodynamic parameters using Spearman correlation analysis. All statistical analyses were performed using IBM SPSS Statistics ver. 20.0 (IBM Co., Armonk, NY, USA). A P-value of <0.05 indicated a significant difference.
RESULTS
Baseline clinical characteristics and urodynamic parameters of the 25 men with a mean age of 67.5±4.6 years, and the comparison between the BOO with DU group (n=10) and the BOO without DU group (n=15) are presented in the Table 1. Clinical characteristics such as age, prostate volume, and symptom scores were not different significantly between the 2 groups. BOO with DU group had larger maximum cystometric capacity (MCC), lower BCI and lower BOO grade than those in the BOO without DU group but maximum flow rate (Qmax) and postvoid residual urine volume were not different between the 2 groups.

Baseline characteristics of enrolled patients
The eNOS level positively correlated with the Qmax (r=0.499, P=0.021) and with MCC (r=0.548, P=0.006). The iNOS level positively correlated with MCC only (r=0.483, P=0.017). The nNOS level positively correlated with the detrusor pressure at Qmax (r=0.626, P=0.048) and with BCI (r=0.609, P=0.022) in all patients (Table 2).

Correlation of eNOS, iNOS, and nNOS with urodynamic parameters
When the expression levels of each isoform of NOS were compared between the BOO with DU and BOO without DU groups, the levels of eNOS (4.052±1.139 vs. 1.863±1.316, P=0.073), iNOS (7.042 ±2.178 vs. 3.869 ±0.687, P =0.347), and nNOS (0.041±0.012 vs. 0.351±0.096, P=0.067) did not significantly differ between the 2 groups (Fig. 1). Immunofluorescence staining revealed that eNOS, iNOS, and nNOS were localized in the urothelium. However, no significant differences were found in the immunofluorescence signals evaluated using image analysis between the BOO without DU and BOO with DU groups (Fig. 2).
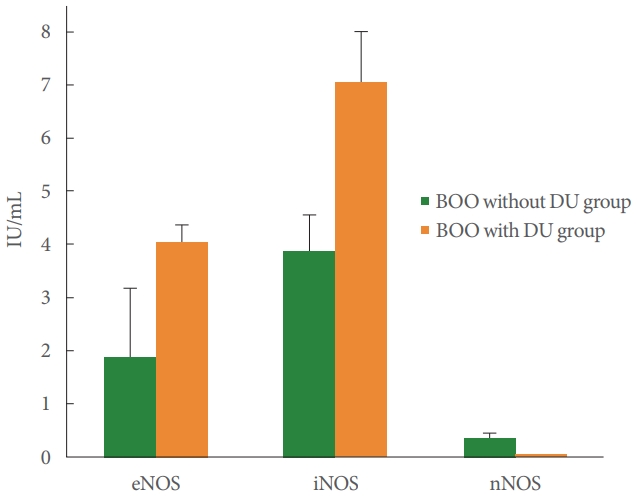
Comparisons of eNOS, iNOS, and nNOS expression levels between the BOO with DU group and BOO without DU group. Data expressed as mean±standard error of the mean. eNOS, endothelial nitric oxide synthase; iNOS, inducible nitric oxide synthase; nNOS, neuronal nitric oxide synthase; BOO, bladder outlet obstruction; DU, detrusor underactivity.
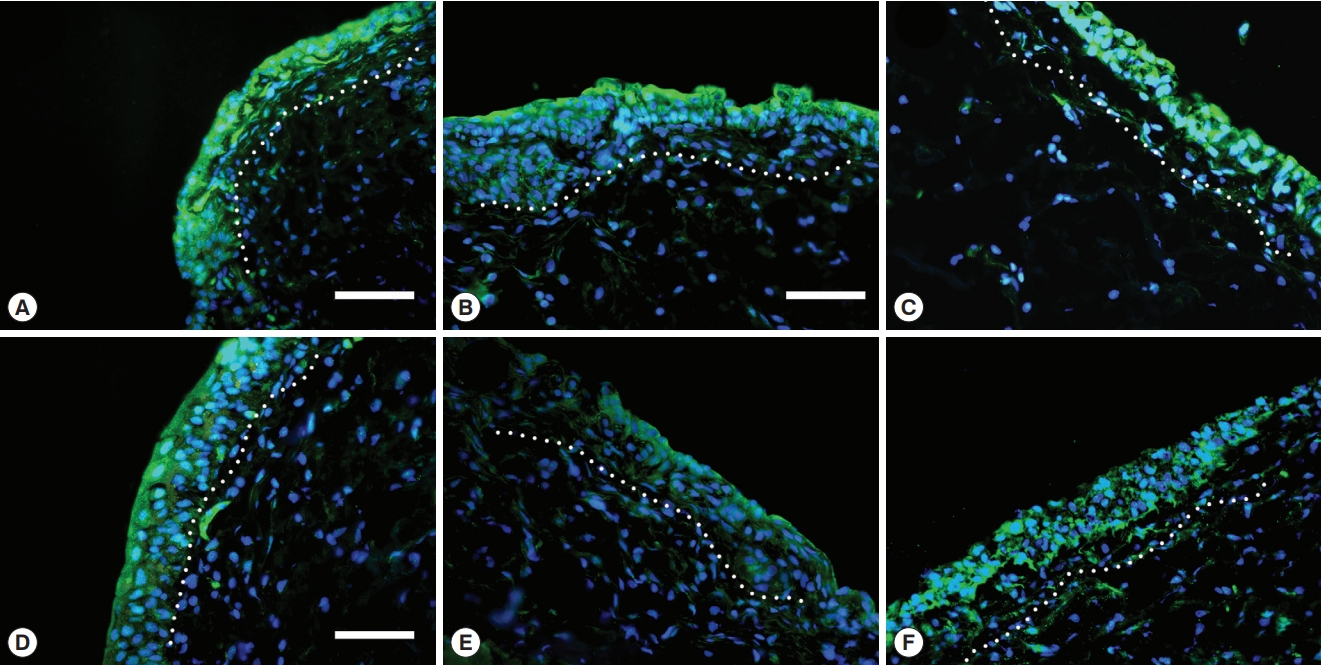
Immunofluorescence staining of eNOS, iNOS, and nNOS. (A–C) eNOS, iNOS, nNOS expressions in the bladder tissues in the BOO with DU group, (D–F) eNOS, iNOS, nNOS expressions in the BOO without DU group. Scale bars: 50 µm, White dotted line separates urothelium from lamina propria. eNOS, endothelial nitric oxide synthase; iNOS, inducible nitric oxide synthase; nNOS, neuronal nitric oxide synthase; BOO, bladder outlet obstruction; DU, detrusor underactivity.
DISCUSSION
We identified the relationship between the urodynamic parameters in men with BOO and the expression of 3 different NOS isoforms that produce NO in the urothelium. The urothelium consolidates sensory information and reflects changes in bladder function. Thus, changes in neurotransmitters in the urothelium have been a focus of studies on new diagnostic markers for bladder dysfunction [10]. Moreover, a significant change in the expression of adenosine triphosphate in the urothelium of patients with DU was observed, on the basis of urodynamic parameters, although eNOS did not show a statistically significant relationship to detrusor function in our previous study [9]. Because we could not identify the change in eNOS with the change in detrusor function despite evidences that urothelial NO could reflect bladder dysfunction [6,7,11], we attempted to investigate the relationship between NO and bladder function using all 3 NOS isoforms in a new set of patients. In the current investigation, we found that the level of eNOS positively correlated with Qmax and with MCC, and the level of iNOS positively correlated with MCC. The relation to Qmax or MCC alone cannot sufficiently reflect the change in bladder function. Although it is difficult to clearly explain the reasons for the correlations of eNOS with Qmax and MCC, which have not been reported in previous studies, they were likely caused by differences in the clinical characteristics of the enrolled patients, especially the symptom severity. Even though we have not directly compared the clinical characteristics in this study population with those of our previous study [9], there would be differences in urodynamics, such as the mean bladder outlet obstruction index, which was 47.4 in this study but it was less than 40 in our previous study. Further studies are needed to identify NOS isoform changes due to these clinical symptom differences.
Increased expression of eNOS in the presence of bladder hyperactivity related to the cyclophosphamide-induced cystitis was reported in an animal study [12], whereas decreased expression of eNOS in the presence of DU, which leads to decreased sensory proteins, was reported in a human study [13]. However, in our study in patients with DU, no significant differences in eNOS and iNOS expression were found.
One study showed that a decrease in iNOS was related to improvement of functional and fibrotic changes in the bladder of rats with BOO [14]. However, another study demonstrated that selective inhibition of iNOS was related to a decrease in bladder capacity, although it did not significantly decrease of bladder weight in mice with BOO. Conversely, the inhibition of all 3 NOS isoforms has been reported to increase nonvoiding contractions and to decrease the bladder capacity [15], thereby worsening the bladder function. Thus, only iNOS could not reflect bladder changes.
In this study, the expression of nNOS in the urothelium of men with BOO positively correlated with the detrusor pressure at Qmax and with BCI, which reflects bladder contractility. nNOS is one of the neurotransmitters released by afferent nerves in the bladder, and changes in nNOS suggest alterations in the afferent system [16]. Hu et al. [17] reported the change in nNOS-positive neurons according to the duration of partial BOO and change in bladder weight in an animal model. In another study, nNOS-positive neurons in partial BOO were decreased by NOS inhibitor administration and increased by L-arginine, which is a substrate for NO formation [18]. These findings suggest that changes in nNOS due to bladder morphological changes induced by BOO cannot sufficiently reflect the changes in nNOS resulting from changes in bladder function. Hannan et al. [19] observed a decrease in nerve terminals expressing nNOS at 1 month after injury in a rat model of bladder dysfunction induced by bilateral pelvic nerve injury, indicating that nNOS is related to impaired bladder function. Another study showed that NO derived from stimulated nNOS increased detrusor activity in the bladder of cats, by demonstrating increased time to onset of spontaneous detrusor contractions and decreased frequency of detrusor contractions due to nNOS inhibition [20]. This was a different effect compared with that of eNOS which decreased bladder activity in the same study.
Other animal studies have shown that anticholinergics that can decrease the frequency of urination could increase nNOS expression and decrease iNOS expression in the bladder wall [21]. Significant increased eNOS and nNOS expressions were reported in the bladder of rat with DO induced by BOO too [22]. Although the comparative indicators of bladder function were not exactly the same, these nNOS and iNOS expression changes were different from the findings of our study, and the reasons for this difference are still unclear.
No significant differences in nNOS were found between the presence and absence of DU, although nNOS correlated with the urodynamic parameters related to the bladder contraction in this study. This may be because DU was defined as BCI < 100 in urodynamics. Although this criterion has been used in previous studies [2,23] and in clinical settings, the value of this urodynamic criterion for distinguishing DU remains unclear. In particular, it could be a limitation of urodynamics, as reflected by our findings.
This study had some limitations. We could not include a control group without BOO in this study because it was difficult to obtain bladder tissue from healthy people. However, men with BOO may have different bladder function status and different values of urodynamic parameters depending on the duration or severity of obstruction. Thus, changes in NOS isoforms can be predicted according to bladder function through a correlation analysis between urodynamic parameters in patients with BOO and the expression levels of NOS. Our study also had technical limitations, one of which is that specimens contained some part of the lamina propria because it is technically difficult to isolate urothelial tissue without including the lamina propria. Therefore, our findings might include the expression of some NOS isoforms in the lamina propria. Another limitation of our study was that we enrolled a relatively small number of patients that was not reached the target number of sample size in the BOO with DU group and did not differentiate between the presence and absence of DO. In addition, it is difficult to distinguish whether the change in NO production is due to passive results associated with BOO or the regulation of NO production as a biological reaction only by comparing the changes in the expression of NOS. Further studies with more patients are needed to elucidate the relevance of changes in the lower urinary tract function to changes in NOS expression levels over the time in patients with BOO. It can supplement previous studies showing discrepant findings on the relationship between NOS and bladder function, which might be due to the lack of evidence from human studies.
In this study, the relationship between NO in the urothelium and bladder function was analyzed by assessing the correlation between NOS expression and urodynamic parameters in men with BOO. The results suggest that nNOS is related to detrusor contractility, however we cannot apply this result to actual clinical practice right away. If further research such as identification of the relationship between NOS isoforms expression in the urothelium and in the urine is carried out, we can used NOS isoforms as a simple, less invasive and more accurate diagnostic tool in the clinical practice.
Notes
Funding Support
This study was supported by the Institute of Clinical Medicine Research of Bucheon St. Mary’s Hospital, Research Fund.
Research Ethics
This study was performed in accordance with the guidelines of the Declaration of Helsinki, and approved by the ethics committee and the institutional review board at our center (HIRB-20170925-035). All patients provided written informed consent before enrollment.
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTION STATEMENT
·Conceptualization JCK
·Data curation: JSK
·Formal analysis: JBC
·Funding acquisition: KJC
·Methodology: KJC, SHP, WSL
·Project administration: KJC
·Visualization: JSK
·Writing-original draft: KJC
·Writing-review & editing: KJC