Urodynamic and Bladder Diary Factors Predict Overactive Bladder-wet in Women: A Comparison With Overactive Bladder-dry
Article information

Abstract
Purpose
To identify factors predicting the presence of overactive bladder syndrome (OAB)-wet, compared with OAB-dry.
Methods
Between September 2007 and September 2013, the medical records of 623 women with OAB who completed a 3-day bladder diary and underwent urodynamic studies in a medical center were retrospectively reviewed. OAB-wet was diagnosed in patients who complained of at least one episode of urgency incontinence in the previous month; otherwise, OAB-dry was diagnosed. Multivariable logistic regression analysis was used to predict the presence of OAB-wet.
Results
Age (odds ratio [OR], 1.05; P<0.001), maximal flow rate (Qmax) (OR,1.06; P<0.001), voided volume (OR, 0.996; P=0.001), detrusor pressure at maximal flow rate (PdetQmax) (OR, 1.02; P=0.003), urgency episodes (OR, 1.04; P<0.001) and urodynamic stress incontinence (OR,1.78; P=0.01) were independent predictors for the presence of OAB-wet vs. OAB-dry. If we use bladder contractility index as a variable for multivariable logistic regression analysis, bladder contractility index (OR, 1.012; P<0.001) become an independent predictor for OAB-wet.
Conclusions
A smaller bladder capacity and more frequent urgency episodes were predictors of OAB-wet, and the above findings indicate that OAB-wet and OAB-dry might be a continuum of OAB. Old age, high Qmax, high PdetQmax and urodynamic stress incontinence were also predictors for OAB-wet, and the above results reveal that OAB-wet and OAB-dry have partially different clinical and urodynamic features. Further studies might be performed to elucidate whether different treatment strategies between OAB-dry and OAB-wet can improve treatment efficacy.
INTRODUCTION
The definition of overactive bladder syndrome (OAB) is urinary urgency, with or without urgency urinary incontinence, which is usually accompanied by urinary frequency and nocturia in the absence of urinary tract infection or other obvious pathologies [1].
OAB can be subclassified as OAB-dry or OAB-wet [2], with an approximate ratio of 2 to 1 [3], and the prevalence of OAB-wet increases with advancing age [4]. However, the underlying pathophysiology of OAB-dry vs. OAB-wet may be different. Kuo et al. [5] reported that urinary nerve growth factor levels are increased in OAB-wet but not OAB-dry. Hsiao et al. [6] reported that C-reactive protein levels are increased in OAB-wet. Hashim and Abrams [7] reported 44% of women with OAB-dry had detrusor overactivity (DO), while 58% of women with OAB-wet had DO. Al-Ghazo et al. [8] also reported 61% of women with OAB-dry had DO, while 69.8% of women with OAB-wet had DO. It has been reported that many patients labeled as OAB-dry may actually be mild OAB-wet [2].
Currently, treatments for OAB-dry vs. OAB-wet patients are nearly the same [9]. Nonetheless, for intravesical injection of onabotulinumtoxinA, OAB-wet patients are associated better therapeutic efficacy [10]. Balzarro et al. [11] also confirmed the efficacy of intravesical injection of onabotulinumtoxinA for treatment of women with OAB-wet. An Urgency Severity Scale score of 4 is OAB-wet, and it was reported that OAB patients with high Urgency Severity Scale score were associated with better therapeutic efficacy after solifenacin treatment [12,13].
Different underlying pathophysiologies may benefit from different treatments. We are interested in whether there is a different underlying pathophysiology in OAB-dry vs. OAB-wet. Comparison of clinical and urodynamic variables between OAB-dry and OAB-wet might be helpful for understanding the underlying pathophysiology. Thus, the aim of this study was to identify clinical and urodynamic factors predicting OAB-wet, compared with OAB-dry.
MATERIALS AND METHODS
Between September 2007 and September 2013, the medical records of consecutive 623 women with OAB who completed a 3-day bladder diary and underwent urodynamic studies at the urogynecologic outpatient clinics of the Department of Obstetrics and Gynecology of a medical center were retrospectively reviewed. OAB was defined as the presence of urinary urgency, with or without urgency incontinence, which is usually accompanied by urinary frequency and nocturia [1]. This study was approved by the Research Ethics Committee in our hospital. Besides, this study has been registered at ClinicalTrials.gov.
The following inclusion criteria were used: (1) women at least 18 years old, who had at least a 3-month history of OAB symptoms, including urgency, urinary frequency, nocturia, or urge incontinence and (2) an average of ≥8 micturitions in 24 hours [14,15]. The exclusion criteria included dominant symptoms with stress urinary incontinence, regular urethral catheterization or intermittent self-catheterization, urinary tract infection or chronic inflammation in the previous 2 weeks, bladder calculus, neurogenic bladder due to radical hysterectomy or injury of central nervous system, and a history of pelvic radiotherapy or a preexisting malignant pelvic tumor. In the study of Stewart et al. [16], OAB-dry was defined as patients who had ≥4 urgency episodes in the past 4 weeks; and OAB-wet was defined as patients who complained of ≥3 urgency incontinence episodes in the past 4 weeks. However, in our study, OAB-wet was diagnosed in patients who complained of at least one episode of urgency incontinence in the previous month; otherwise, OAB-dry was diagnosed.
The medical history, including information such as age and parity, was reviewed for each patient. The urodynamic assessment included uroflowmetry, filling cystometry with 35°C distilled water at a rate of 60 mL/sec, a pressure flow study, and the stress urethral pressure profile with patient in sitting position [17]. Additionally, a 20-minute pad test for each woman was performed [18,19]. DO was defined as evidence of spontaneous detrusor contractions occurring during bladder filling or an uninhibited detrusor contraction occurring at a cystometric capacity that usually results in voiding [20]. If patients had a strong desire to void at a volume less than 300 mL, they were considered to have bladder oversensitivity [21]. Functional bladder outlet obstruction (BOO) was defined as uroflowmetry results <15-mL/sec maximal flow rate (Qmax) and >20-cm H2O detrusor pressure at maximal flow rate (PdetQmax) measured via voiding cystometry and without a known anatomic cause of obstruction [22,23].
Multichannel urodynamic equipment (Life-Tech, Houston, TX, USA) with computer analysis and Urovision (Urolab Janus System V, Houston) was used. All terminology conformed to the standards recommended by the International Continence Society and Urodynamic Society [1]. All procedures were performed by an experienced technician, and the data were interpreted by a single observer to avoid interobserver variability.
STATA ver. 11.0 (Stata Corp., College Station, TX, USA) was used for statistical analyses. The chi-square test and Wilcoxon rank-sum test were used as appropriate. A P-value of less than 0.05 was considered statistically significant. A multivariable logistic regression analysis was performed using variables that had a P-value <0.05 from the univariate analysis [24].
RESULTS
One hundred twenty-seven women with OAB-wet and 496 women with OAB-dry were enrolled in this study. Comparisons of age, parity, pad weights, and urodynamic and bladder diary parameters between the OAB-wet and OAB-dry groups are shown in Tables 1 and 2. Age and parity were significantly different between the OAB-wet and OAB-dry groups (Table 1). After adjusting for age and parity, we found that Qmax, voided volume, PdetQmax, urodynamic stress incontinence (USI), pad weight, urgency episodes, incontinence episodes, and bladder contractility index (i.e.,=PdetQmax+5×Qmax) [25] were significantly different between the OAB-wet and OAB-dry groups (Tables 1, 2).

Comparisons of the urodynamic parameters between the OAB-wet and OAB-dry groups (n=623)
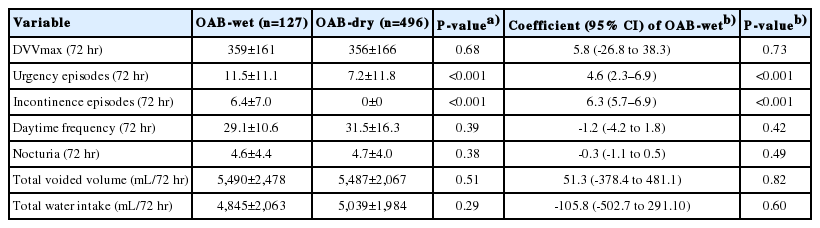
Comparisons of the bladder diary parameters between the OAB-wet and OAB-dry groups (n=623)
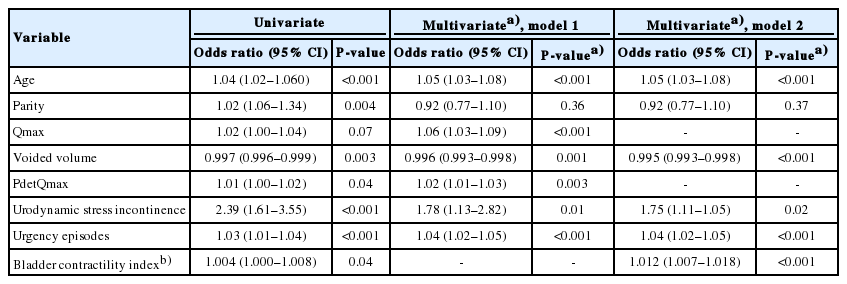
Because pad weight was highly correlated to USI (Spearman rho=0.88, P<0.0001), pad weight was not included in the multivariable analysis (Table 2). In addition, incontinence episodes >0 predicted OAB-wet perfectly, therefore, we excluded the variable “incontinence episodes” in the multivariable analysis (Table 2). In model 1, using age, parity and the other statistically significant adjusted variables shown in Tables 1 and 2, a multivariable logistic regression was performed to predict OAB-wet (Table 3). Age (odds ratio [OR],1.05; P<0.001), Qmax (OR, 1.06; P<0.001), voided volume (OR, 0.996; P=0.001), PdetQmax (OR, 1.02; P=0.003), USI (OR, 1.78; P=0.01), and urgency episodes (OR, 1.04; P<0.001) were independent predictors for OAB-wet vs. OAB-dry (Table 3). In model 2, bladder contractility index was included as a variable for multivariable logistic regression to predict OAB-wet, instead of using Qmax and PdetQmax as variables (Table 3); bladder contractility index (OR, 1.012; P<0.0001) was found to be an independent predictor for OAB-wet (Table 3).
Factors predicting women with OAB-wet using univariate and multivariable logistic regressi
DISCUSSION
Compared with OAB-dry, a smaller voided volume (OR, 0.996) and higher urgency episodes (OR, 1.04) were found to be predictors of OAB-wet (Table 3). Al-Zahrani and Gajewski [26] reported that as overactive bladder symptoms increase in severity, female patients tend to have a smaller bladder capacity. Urgency is the core symptom of female OAB [27], and Giarenis et al. [28] found a negative correlation between urgency episodes and bladder capacity in women with idiopathic DO. Thus, together with our findings, the speculation of OAB-wet as a severe form of OAB seems reasonable.
Cho et al. [29] reported similar Qmax (mean: 15.3 mL/sec vs. 15.0 mL/sec, P=0.759) and PdetQmax (mean: 31.0 cm H2O vs. 31.4 cm H2O, P=0.862) between the OAB-dry and OAB-wet patients. In our study, high Qmax (OR, 1.06) and high PdetQmax (OR, 1.01) were identified as novel predictors for OAB-wet (Table 3). Furthermore, bladder contractility index (i.e.,=PdetQmax +5×Qmax) [25] (OR, 1.012, P<0.001) is an independent predictor for OAB-wet (Table 3). Thus, our findings of high Qmax, high PdetQmax, and high bladder contractility index as predictors of OAB-wet may hint that the bladder contractility is better for OAB-wet, compared with OAB-dry.
Old age (OR, 1.04) is another predictor for OAB-wet (Table 3). Chen et al. [4] reported that the prevalence of OAB-wet increased with advancing age. Tyagi et al. [30] reported a significant association between OAB symptoms and age (OR,1.12). Hung et al. [27] also reported that women with OAB-wet had a greater average age.
In our study, USI was a predictor for OAB-wet, and women with OAB-wet had a higher incidence of coexistent USI, vs. OAB-dry (54.3% vs. 33.5%, P<0.001) (Table 1). From the ambulatory urodynamic monitoring data of Dokmeci et al. [31], the rate of stress urinary incontinence in OAB-wet also had a trend to be higher than OAB-dry (72.5% vs. 52.8%, P=0.075). From the above, if the clinical works for treating OAB-wet resulted in poor therapeutic response, then combined treatment for the coexistence of USI might be considered in clinical practice.
Nowadays, treatments for OAB-wet vs. OAB-dry patients are nearly the same [9]. However, from our results, OAB-wet women have different clinical presentations, such as greater severity in symptoms, greater bladder contractility and higher coexistent USI rate, compared with OAB-dry (Table 3). Thus, pretreatment assessment or treatment strategies might be different for OAB-wet vs. OAB-dry. For example, urodynamic studies to unmask USI might be indicated for OAB-wet women with poor response to pharmacotherapy [32]; higher starting dose for the treatment of OAB might be more suitable for OAB-wet; for the indication of intravesical injection of onabotulinumtoxinA [10,32], OAB-wet patients should be more suitable than OAB-dry [10]. Future prospective clinical studies should be performed to find the most suitable treatment strategy for OAB-wet vs. OAB-dry patients.
The retrospective design of this study was a limitation; however, the large sample size should make our data reliable. Besides, we do not have the posttreatment data. Further studies may be performed to elucidate post-treatment differences between OAB-dry and OAB-wet. In addition, we do not have long-term follow-up data; future long-term follow-up studies may be performed to clarify the relationship between OAB-dry and OAB-wet.
In conclusion, a smaller bladder capacity and more frequent urgency episodes were predictors of OAB-wet, and the above findings indicate that OAB-wet and OAB-dry might be a continuum of OAB. Old age, high Qmax, high PdetQmax, and USI were also independent predictors for OAB-wet, and the above results indicate that OAB-wet and OAB-dry have partially different clinical and urodynamic features. Further studies may be performed to elucidate whether different treatment strategies between OAB-dry and OAB-wet could improve treatment efficacy.
Notes
Research Ethics
This study was approved by the Research Ethics Committee in National Taiwan University Hospital (approval number: 201404012RINC). Besides, this study has been registered at ClinicalTrials.gov (NCT03560778). The informed consents were not obtained due to that this is a retrospective study and the data were analyzed anonymously, and the National Taiwan University Hospital Research Ethics Committee waived the need for informed consent form the participants.
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTION STATEMENT
· Full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis: SMH, HHL
· Study concept and design: HHL
· Acquisition of data: TCC, CHC
· Analysis and interpretation of data: SMH
· Drafting of the manuscript: SMH, PCW
· Critical revision of the manuscript for important intellectual content: HHL
· Statistical analysis: SMH
· Obtained funding: HHL
· Administrative, technical, or material support: HHL
· Study supervision: HHL